Pieter A. van Doorn, Peter Y. K. Van den Bergh, Robert D. M. Hadden, Bert Avau, Patrik Vankrunkelsven, Shahram Attarian, Patricia H. Blomkwist-Markens, David R. Cornblath, H. Stephan Goedee, Thomas Harbo, Bart C. Jacobs, Susumu Kusunoki, Helmar C. Lehmann, Richard A. Lewis, Michael P. Lunn, Eduardo Nobile-Orazio, Luis Querol, Yusuf A. Rajabally, Thirugnanam Umapathi, Haluk A. Topaloglu, Hugh J. Willison
{"title":"European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain–Barré syndrome","authors":"Pieter A. van Doorn, Peter Y. K. Van den Bergh, Robert D. M. Hadden, Bert Avau, Patrik Vankrunkelsven, Shahram Attarian, Patricia H. Blomkwist-Markens, David R. Cornblath, H. Stephan Goedee, Thomas Harbo, Bart C. Jacobs, Susumu Kusunoki, Helmar C. Lehmann, Richard A. Lewis, Michael P. Lunn, Eduardo Nobile-Orazio, Luis Querol, Yusuf A. Rajabally, Thirugnanam Umapathi, Haluk A. Topaloglu, Hugh J. Willison","doi":"10.1111/jns.12594","DOIUrl":null,"url":null,"abstract":"<p>Guillain–Barré syndrome (GBS) is an acute polyradiculoneuropathy. Symptoms may vary greatly in presentation and severity. Besides weakness and sensory disturbances, patients may have cranial nerve involvement, respiratory insufficiency, autonomic dysfunction and pain. To develop an evidence-based guideline for the diagnosis and treatment of GBS, using Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology, a Task Force (TF) of the European Academy of Neurology (EAN) and the Peripheral Nerve Society (PNS) constructed 14 Population/Intervention/Comparison/Outcome questions (PICOs) covering diagnosis, treatment and prognosis of GBS, which guided the literature search. Data were extracted and summarised in GRADE Summaries of Findings (for treatment PICOs) or Evidence Tables (for diagnostic and prognostic PICOs). Statements were prepared according to GRADE Evidence-to-Decision (EtD) frameworks. For the six intervention PICOs, evidence-based recommendations are made. For other PICOs, good practice points (GPPs) are formulated. For diagnosis, the principal GPPs are: GBS is more likely if there is a history of recent diarrhoea or respiratory infection; CSF examination is valuable, particularly when the diagnosis is less certain; electrodiagnostic testing is advised to support the diagnosis; testing for anti-ganglioside antibodies is of limited clinical value in most patients with typical motor-sensory GBS, but anti-GQ1b antibody testing should be considered when Miller Fisher syndrome (MFS) is suspected; nodal–paranodal antibodies should be tested when autoimmune nodopathy is suspected; MRI or ultrasound imaging should be considered in atypical cases; and changing the diagnosis to acute-onset chronic inflammatory demyelinating polyradiculoneuropathy (A-CIDP) should be considered if progression continues after 8 weeks from onset, which occurs in around 5% of patients initially diagnosed with GBS. For treatment, the TF recommends intravenous immunoglobulin (IVIg) 0.4 g/kg for 5 days, in patients within 2 weeks (GPP also within 2–4 weeks) after onset of weakness if unable to walk unaided, or a course of plasma exchange (PE) 12–15 L in four to five exchanges over 1–2 weeks, in patients within 4 weeks after onset of weakness if unable to walk unaided. The TF recommends against a second IVIg course in GBS patients with a poor prognosis; recommends against using oral corticosteroids, and weakly recommends against using IV corticosteroids; does not recommend PE followed immediately by IVIg; weakly recommends gabapentinoids, tricyclic antidepressants or carbamazepine for treatment of pain; does not recommend a specific treatment for fatigue. To estimate the prognosis of individual patients, the TF advises using the modified Erasmus GBS outcome score (mEGOS) to assess outcome, and the modified Erasmus GBS Respiratory Insufficiency Score (mEGRIS) to assess the risk of requiring artificial ventilation. Based on the PICOs, available literature and additional discussions, we provide flow charts to assist making clinical decisions on diagnosis, treatment and the need for intensive care unit admission.</p>","PeriodicalId":17451,"journal":{"name":"Journal of the Peripheral Nervous System","volume":"28 4","pages":"535-563"},"PeriodicalIF":3.2000,"publicationDate":"2023-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jns.12594","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Peripheral Nervous System","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jns.12594","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
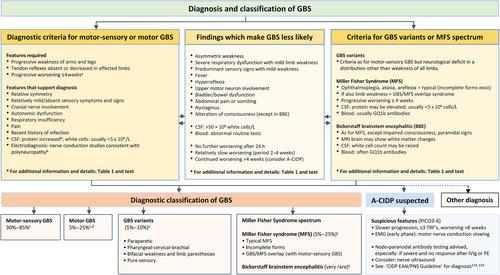
Guillain–Barré syndrome (GBS) is an acute polyradiculoneuropathy. Symptoms may vary greatly in presentation and severity. Besides weakness and sensory disturbances, patients may have cranial nerve involvement, respiratory insufficiency, autonomic dysfunction and pain. To develop an evidence-based guideline for the diagnosis and treatment of GBS, using Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology, a Task Force (TF) of the European Academy of Neurology (EAN) and the Peripheral Nerve Society (PNS) constructed 14 Population/Intervention/Comparison/Outcome questions (PICOs) covering diagnosis, treatment and prognosis of GBS, which guided the literature search. Data were extracted and summarised in GRADE Summaries of Findings (for treatment PICOs) or Evidence Tables (for diagnostic and prognostic PICOs). Statements were prepared according to GRADE Evidence-to-Decision (EtD) frameworks. For the six intervention PICOs, evidence-based recommendations are made. For other PICOs, good practice points (GPPs) are formulated. For diagnosis, the principal GPPs are: GBS is more likely if there is a history of recent diarrhoea or respiratory infection; CSF examination is valuable, particularly when the diagnosis is less certain; electrodiagnostic testing is advised to support the diagnosis; testing for anti-ganglioside antibodies is of limited clinical value in most patients with typical motor-sensory GBS, but anti-GQ1b antibody testing should be considered when Miller Fisher syndrome (MFS) is suspected; nodal–paranodal antibodies should be tested when autoimmune nodopathy is suspected; MRI or ultrasound imaging should be considered in atypical cases; and changing the diagnosis to acute-onset chronic inflammatory demyelinating polyradiculoneuropathy (A-CIDP) should be considered if progression continues after 8 weeks from onset, which occurs in around 5% of patients initially diagnosed with GBS. For treatment, the TF recommends intravenous immunoglobulin (IVIg) 0.4 g/kg for 5 days, in patients within 2 weeks (GPP also within 2–4 weeks) after onset of weakness if unable to walk unaided, or a course of plasma exchange (PE) 12–15 L in four to five exchanges over 1–2 weeks, in patients within 4 weeks after onset of weakness if unable to walk unaided. The TF recommends against a second IVIg course in GBS patients with a poor prognosis; recommends against using oral corticosteroids, and weakly recommends against using IV corticosteroids; does not recommend PE followed immediately by IVIg; weakly recommends gabapentinoids, tricyclic antidepressants or carbamazepine for treatment of pain; does not recommend a specific treatment for fatigue. To estimate the prognosis of individual patients, the TF advises using the modified Erasmus GBS outcome score (mEGOS) to assess outcome, and the modified Erasmus GBS Respiratory Insufficiency Score (mEGRIS) to assess the risk of requiring artificial ventilation. Based on the PICOs, available literature and additional discussions, we provide flow charts to assist making clinical decisions on diagnosis, treatment and the need for intensive care unit admission.
期刊介绍:
The Journal of the Peripheral Nervous System is the official journal of the Peripheral Nerve Society. Founded in 1996, it is the scientific journal of choice for clinicians, clinical scientists and basic neuroscientists interested in all aspects of biology and clinical research of peripheral nervous system disorders.
The Journal of the Peripheral Nervous System is a peer-reviewed journal that publishes high quality articles on cell and molecular biology, genomics, neuropathic pain, clinical research, trials, and unique case reports on inherited and acquired peripheral neuropathies.
Original articles are organized according to the topic in one of four specific areas: Mechanisms of Disease, Genetics, Clinical Research, and Clinical Trials.
The journal also publishes regular review papers on hot topics and Special Issues on basic, clinical, or assembled research in the field of peripheral nervous system disorders. Authors interested in contributing a review-type article or a Special Issue should contact the Editorial Office to discuss the scope of the proposed article with the Editor-in-Chief.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


