Self-expanding metal stents versus decompression tubes as a bridge to surgery for patients with obstruction caused by colorectal cancer: a systematic review and meta-analysis.
Wei Ma, Jian-Cheng Zhang, Kun Luo, Lu Wang, Chi Zhang, Bin Cai, Hua Jiang
{"title":"Self-expanding metal stents versus decompression tubes as a bridge to surgery for patients with obstruction caused by colorectal cancer: a systematic review and meta-analysis.","authors":"Wei Ma, Jian-Cheng Zhang, Kun Luo, Lu Wang, Chi Zhang, Bin Cai, Hua Jiang","doi":"10.1186/s13017-023-00515-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Using self-expanding metal stents (SEMS) and decompression tubes (DT) as a bridge-to-surgery (BTS) treatment may avoid emergency operations for patients with colorectal cancer-caused obstructions. This study aimed to evaluate the efficacy and safety of the two approaches.</p><p><strong>Methods: </strong>We systematically retrieved literature from January 1, 2000, to May 30, 2023, from the PubMed, Embase, Web of Science, SinoMed, Wanfang Data, Chinese National Knowledge Infrastructure, and Cochrane Central Register of Clinical Trials databases. Randomized controlled trials (RCTs) or cohort studies of SEMS versus DT as BTS in colorectal cancer obstruction were selected. Risks of bias were assessed for RCTs and cohort studies using the Cochrane Risk of Bias tool version 2 and Risk of Bias in Nonrandomized Studies of Interventions. Certainty of evidence was determined using the Graded Recommendation Assessment. Odds ratio (OR), mean difference (MD), and 95% confidence interval (95% CI) were used to analyze measurement data.</p><p><strong>Results: </strong>We included eight RCTs and eighteen cohort studies involving 2,061 patients (SEMS, 1,044; DT, 1,017). Pooled RCT and cohort data indicated the SEMS group had a significantly higher clinical success rate than the DT group (OR = 1.99, 95% CI 1.04, 3.81, P = 0.04), but no significant difference regarding technical success (OR = 1.29, 95% CI 0.56, 2.96, P = 0.55). SEMS had a shorter postoperative length of hospital stays (MD = - 4.47, 95% CI - 6.26, - 2.69, P < 0.00001), a lower rates of operation-related abdominal pain (OR = 0.16, 95% CI 0.05, 0.50, P = 0.002), intraoperative bleeding (MD = - 37.67, 95% CI - 62.73, - 12.60, P = 0.003), stoma creation (OR = 0.41, 95% CI 0.23, 0.73, P = 0.002) and long-term tumor recurrence rate than DT (OR = 0.47, 95% CI 0.22, 0.99, P = 0.05).</p><p><strong>Conclusion: </strong>SEMS and DT are both safe as BTS to avoid emergency surgery for patients with colorectal cancer obstruction. SEMS is preferable because of higher clinical success rates, lower rates of operation-related abdominal pain, intraoperative bleeding, stoma creation, and long-term tumor recurrence, as well as a shorter postoperative length of hospital stays. Trial registration CRD42022365951 .</p>","PeriodicalId":48867,"journal":{"name":"World Journal of Emergency Surgery","volume":"18 1","pages":"46"},"PeriodicalIF":6.0000,"publicationDate":"2023-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10536785/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13017-023-00515-6","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Using self-expanding metal stents (SEMS) and decompression tubes (DT) as a bridge-to-surgery (BTS) treatment may avoid emergency operations for patients with colorectal cancer-caused obstructions. This study aimed to evaluate the efficacy and safety of the two approaches.
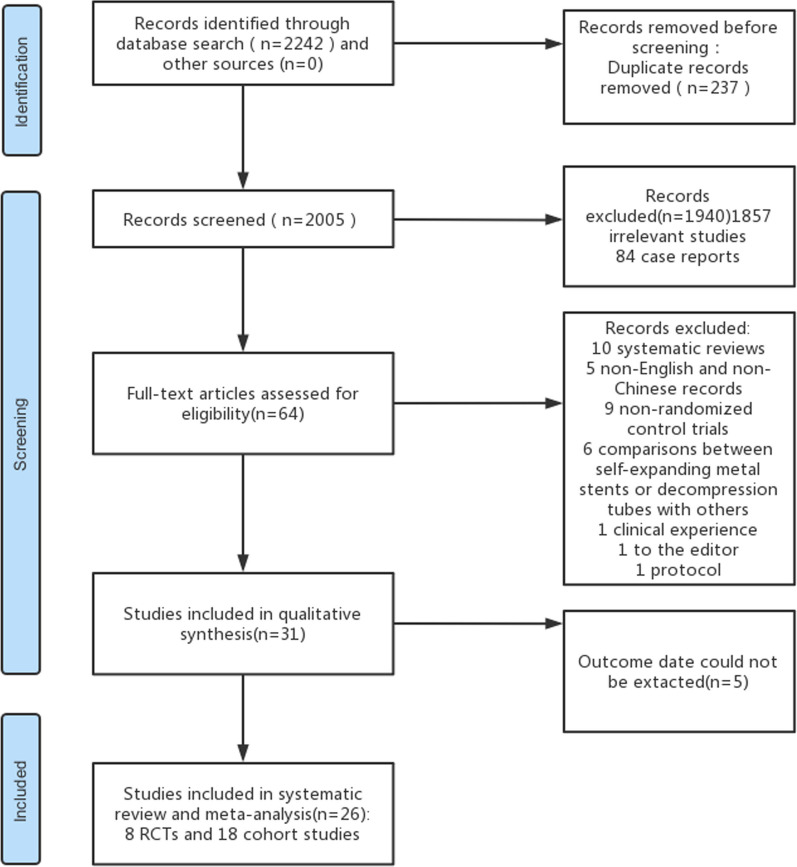
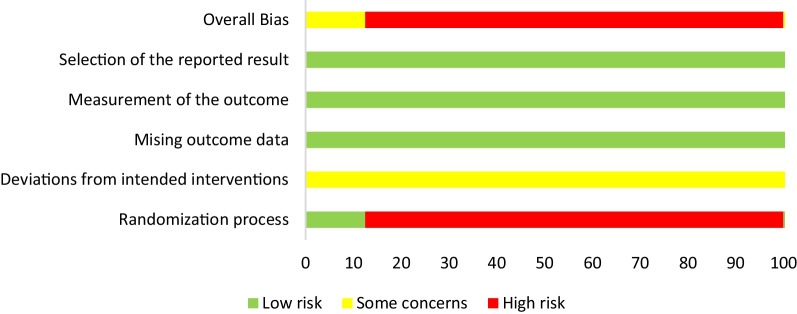
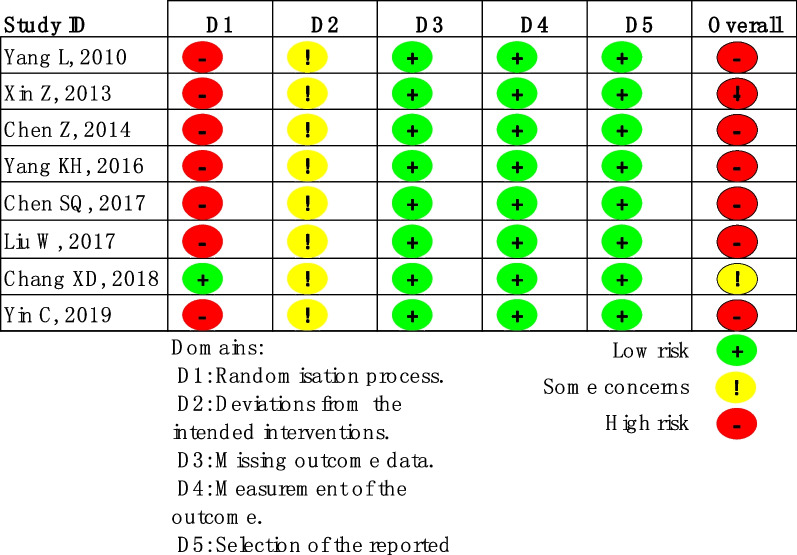
Methods: We systematically retrieved literature from January 1, 2000, to May 30, 2023, from the PubMed, Embase, Web of Science, SinoMed, Wanfang Data, Chinese National Knowledge Infrastructure, and Cochrane Central Register of Clinical Trials databases. Randomized controlled trials (RCTs) or cohort studies of SEMS versus DT as BTS in colorectal cancer obstruction were selected. Risks of bias were assessed for RCTs and cohort studies using the Cochrane Risk of Bias tool version 2 and Risk of Bias in Nonrandomized Studies of Interventions. Certainty of evidence was determined using the Graded Recommendation Assessment. Odds ratio (OR), mean difference (MD), and 95% confidence interval (95% CI) were used to analyze measurement data.
Results: We included eight RCTs and eighteen cohort studies involving 2,061 patients (SEMS, 1,044; DT, 1,017). Pooled RCT and cohort data indicated the SEMS group had a significantly higher clinical success rate than the DT group (OR = 1.99, 95% CI 1.04, 3.81, P = 0.04), but no significant difference regarding technical success (OR = 1.29, 95% CI 0.56, 2.96, P = 0.55). SEMS had a shorter postoperative length of hospital stays (MD = - 4.47, 95% CI - 6.26, - 2.69, P < 0.00001), a lower rates of operation-related abdominal pain (OR = 0.16, 95% CI 0.05, 0.50, P = 0.002), intraoperative bleeding (MD = - 37.67, 95% CI - 62.73, - 12.60, P = 0.003), stoma creation (OR = 0.41, 95% CI 0.23, 0.73, P = 0.002) and long-term tumor recurrence rate than DT (OR = 0.47, 95% CI 0.22, 0.99, P = 0.05).
Conclusion: SEMS and DT are both safe as BTS to avoid emergency surgery for patients with colorectal cancer obstruction. SEMS is preferable because of higher clinical success rates, lower rates of operation-related abdominal pain, intraoperative bleeding, stoma creation, and long-term tumor recurrence, as well as a shorter postoperative length of hospital stays. Trial registration CRD42022365951 .
期刊介绍:
The World Journal of Emergency Surgery is an open access, peer-reviewed journal covering all facets of clinical and basic research in traumatic and non-traumatic emergency surgery and related fields. Topics include emergency surgery, acute care surgery, trauma surgery, intensive care, trauma management, and resuscitation, among others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


