Meena Bhatia, Christopher J Scheiber, Simrat Arora, Chelsea Gustafson, Ian Funk, Craig Grosshuesch, Carter Simmers, Quefeng Li, Yutong Liu, Alan M Smeltz
{"title":"Should All Patients With Pulmonary Hypertension Undergoing Non-Cardiac Surgery Be Managed by Cardiothoracic Fellowship-Trained Anesthesiologists?","authors":"Meena Bhatia, Christopher J Scheiber, Simrat Arora, Chelsea Gustafson, Ian Funk, Craig Grosshuesch, Carter Simmers, Quefeng Li, Yutong Liu, Alan M Smeltz","doi":"10.1177/10892532231203128","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To identify differences in practice patterns and outcomes related to the induction of general anesthesia for patients with pulmonary hypertension (PH) performed by anesthesiologists who have completed a cardiothoracic fellowship (CTA group) vs those who have not (non-CTA group).</p><p><strong>Design: </strong>Retrospective study with propensity score matching.</p><p><strong>Setting: </strong>Operating room.</p><p><strong>Participants: </strong>All adult patients with PH undergoing general anesthesia requiring intubation at a single academic center over 5 years.</p><p><strong>Interventions: </strong>Patient baseline characteristics, peri-induction management variables, post-induction mean arterial pressure (MAP), and other outcomes were compared between CTA and non-CTA groups.</p><p><strong>Methods and main results: </strong>Following propensity scoring matching, 402 patients were included in the final model, 100 in the CTA group and 302 in the non-CTA group. Also following matching, only cases of mild to moderate PH without right ventricular dysfunction remained in the analysis. Matched groups were overall statistically similar with respect to baseline characteristics; however, there was a greater incidence of higher ASA class (<i>P</i> = .025) and cardiology and thoracic procedures (<i>P</i> < .001) being managed by the CTA group. No statistical differences were identified in practice patterns or outcomes related to the induction of anesthesia between groups, except for longer hospital length of stay in the CTA group (<i>P</i> = .008).</p><p><strong>Conclusions: </strong>These results provide early evidence to suggest the induction of general anesthesia of patients with non-severe PH disease can be comparably managed by either anesthesiologists with or without a cardiothoracic fellowship. However, these findings should be confirmed in a prospective study.</p>","PeriodicalId":46500,"journal":{"name":"Seminars in Cardiothoracic and Vascular Anesthesia","volume":" ","pages":"305-312"},"PeriodicalIF":1.0000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10676614/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Cardiothoracic and Vascular Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/10892532231203128","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: To identify differences in practice patterns and outcomes related to the induction of general anesthesia for patients with pulmonary hypertension (PH) performed by anesthesiologists who have completed a cardiothoracic fellowship (CTA group) vs those who have not (non-CTA group).
Design: Retrospective study with propensity score matching.
Setting: Operating room.
Participants: All adult patients with PH undergoing general anesthesia requiring intubation at a single academic center over 5 years.
Interventions: Patient baseline characteristics, peri-induction management variables, post-induction mean arterial pressure (MAP), and other outcomes were compared between CTA and non-CTA groups.
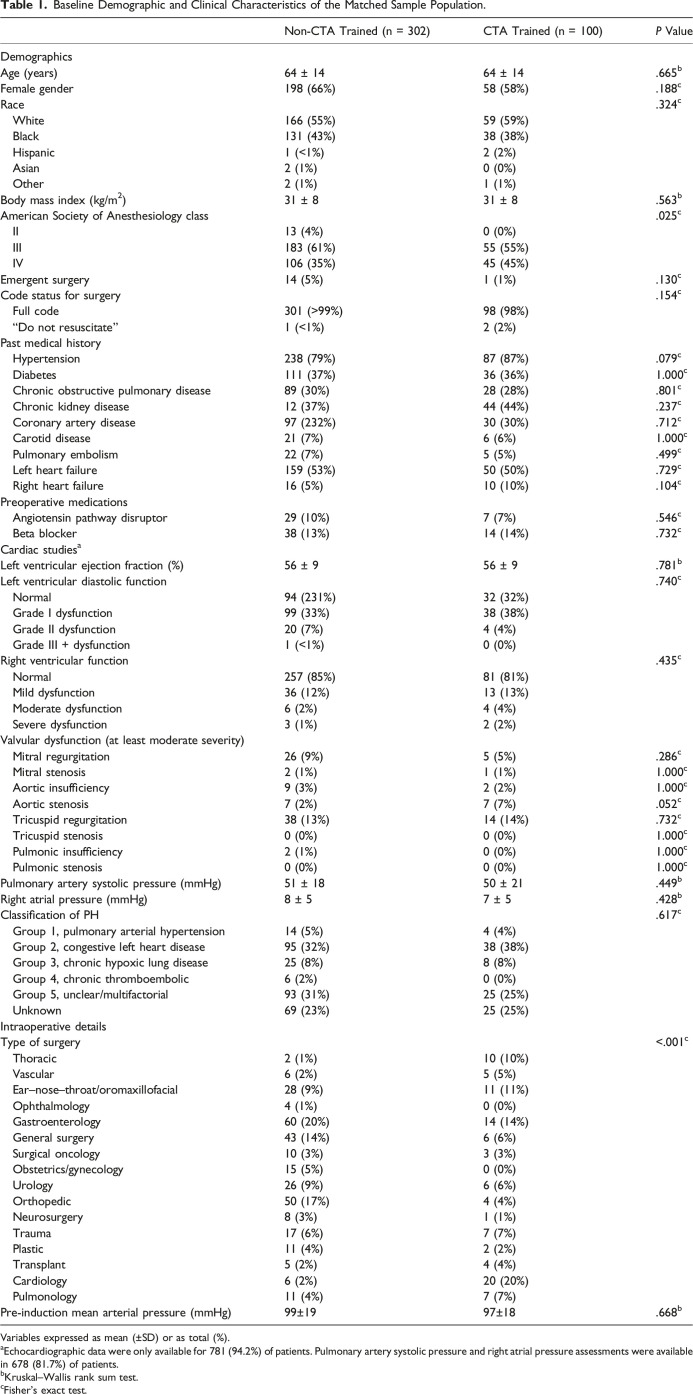
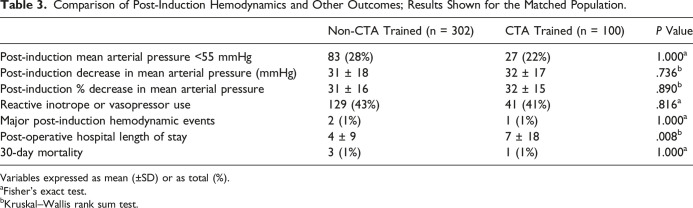
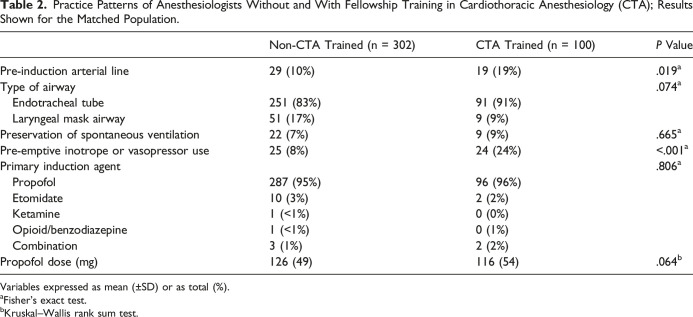
Methods and main results: Following propensity scoring matching, 402 patients were included in the final model, 100 in the CTA group and 302 in the non-CTA group. Also following matching, only cases of mild to moderate PH without right ventricular dysfunction remained in the analysis. Matched groups were overall statistically similar with respect to baseline characteristics; however, there was a greater incidence of higher ASA class (P = .025) and cardiology and thoracic procedures (P < .001) being managed by the CTA group. No statistical differences were identified in practice patterns or outcomes related to the induction of anesthesia between groups, except for longer hospital length of stay in the CTA group (P = .008).
Conclusions: These results provide early evidence to suggest the induction of general anesthesia of patients with non-severe PH disease can be comparably managed by either anesthesiologists with or without a cardiothoracic fellowship. However, these findings should be confirmed in a prospective study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


