Hemant Deepak Shewade, G Kiruthika, Prabhadevi Ravichandran, Swati Iyer, Aniket Chowdhury, S Kiran Pradeep, Kathiresan Jeyashree, S Devika, Joshua Chadwick, Jeromie Wesley Vivian, Dheeraj Tumu, Amar N Shah, Bhavin Vadera, Venkatesh Roddawar, Sanjay K Mattoo, Kiran Rade, Raghuram Rao, Manoj V Murhekar
{"title":"Quality of active case-finding for tuberculosis in India: a national level secondary data analysis.","authors":"Hemant Deepak Shewade, G Kiruthika, Prabhadevi Ravichandran, Swati Iyer, Aniket Chowdhury, S Kiran Pradeep, Kathiresan Jeyashree, S Devika, Joshua Chadwick, Jeromie Wesley Vivian, Dheeraj Tumu, Amar N Shah, Bhavin Vadera, Venkatesh Roddawar, Sanjay K Mattoo, Kiran Rade, Raghuram Rao, Manoj V Murhekar","doi":"10.1080/16549716.2023.2256129","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>India has been implementing active case-finding (ACF) for TB among marginalised and vulnerable (high-risk) populations since 2017. The effectiveness of ACF cycle(s) is dependent on the use of appropriate screening and diagnostic tools and meeting quality indicators.</p><p><strong>Objectives: </strong>To determine the number of ACF cycles implemented in 2021 at national, state (<i>n</i> = 36) and district (<i>n</i> = 768) level and quality indicators for the first ACF cycle.</p><p><strong>Methods: </strong>In this descriptive study, aggregate TB program data for each ACF activity that was extracted was further aggregated against each ACF cycle at the district level in 2021. One ACF cycle was the period identified to cover all the high-risk populations in the district. Three TB ACF quality indicators were calculated: percentage population screened (≥10%), percentage tested among screened (≥4.8%) and percentage diagnosed among tested (≥5%). We also calculated the number needed to screen (NNS) for diagnosing one person with TB (≤1538).</p><p><strong>Results: </strong>Of 768 TB districts, ACF data for 111 were not available. Of the remaining 657 districts, 642 (98%) implemented one, and 15 implemented two to three ACF cycles. None of the districts or states met all three TB ACF quality indicators' cut-offs. At the national level, for the first ACF cycle, 9.3% of the population were screened, 1% of the screened were tested and 3.7% of the tested were diagnosed. The NNS was 2824: acceptable (≤1538) in institutional facilities and poor for population-based groups. Data were not consistently available to calculate the percentage of i) high-risk population covered, ii) presumptive TB among screened and iii) tested among presumptive.</p><p><strong>Conclusion: </strong>In 2021, India implemented one ACF cycle with sub-optimal ACF quality indicators. Reducing the losses between screening and testing, improving data quality and sensitising stakeholders regarding the importance of meeting all ACF quality indicators are recommended.</p>","PeriodicalId":49197,"journal":{"name":"Global Health Action","volume":null,"pages":null},"PeriodicalIF":2.2000,"publicationDate":"2023-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10515680/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Action","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/16549716.2023.2256129","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: India has been implementing active case-finding (ACF) for TB among marginalised and vulnerable (high-risk) populations since 2017. The effectiveness of ACF cycle(s) is dependent on the use of appropriate screening and diagnostic tools and meeting quality indicators.
Objectives: To determine the number of ACF cycles implemented in 2021 at national, state (n = 36) and district (n = 768) level and quality indicators for the first ACF cycle.
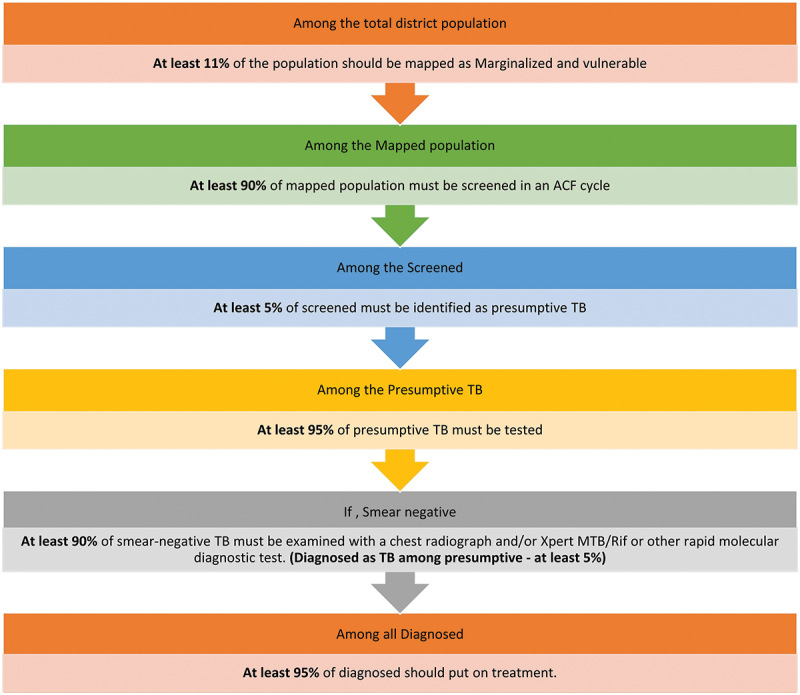
Methods: In this descriptive study, aggregate TB program data for each ACF activity that was extracted was further aggregated against each ACF cycle at the district level in 2021. One ACF cycle was the period identified to cover all the high-risk populations in the district. Three TB ACF quality indicators were calculated: percentage population screened (≥10%), percentage tested among screened (≥4.8%) and percentage diagnosed among tested (≥5%). We also calculated the number needed to screen (NNS) for diagnosing one person with TB (≤1538).
Results: Of 768 TB districts, ACF data for 111 were not available. Of the remaining 657 districts, 642 (98%) implemented one, and 15 implemented two to three ACF cycles. None of the districts or states met all three TB ACF quality indicators' cut-offs. At the national level, for the first ACF cycle, 9.3% of the population were screened, 1% of the screened were tested and 3.7% of the tested were diagnosed. The NNS was 2824: acceptable (≤1538) in institutional facilities and poor for population-based groups. Data were not consistently available to calculate the percentage of i) high-risk population covered, ii) presumptive TB among screened and iii) tested among presumptive.
Conclusion: In 2021, India implemented one ACF cycle with sub-optimal ACF quality indicators. Reducing the losses between screening and testing, improving data quality and sensitising stakeholders regarding the importance of meeting all ACF quality indicators are recommended.
期刊介绍:
Global Health Action is an international peer-reviewed Open Access journal affiliated with the Unit of Epidemiology and Global Health, Department of Public Health and Clinical Medicine at Umeå University, Sweden. The Unit hosts the Umeå International School of Public Health and the Umeå Centre for Global Health Research.
Vision: Our vision is to be a leading journal in the global health field, narrowing health information gaps and contributing to the implementation of policies and actions that lead to improved global health.
Aim: The widening gap between the winners and losers of globalisation presents major public health challenges. To meet these challenges, it is crucial to generate new knowledge and evidence in the field and in settings where the evidence is lacking, as well as to bridge the gaps between existing knowledge and implementation of relevant findings. Thus, the aim of Global Health Action is to contribute to fuelling a more concrete, hands-on approach to addressing global health challenges. Manuscripts suggesting strategies for practical interventions and research implementations where none already exist are specifically welcomed. Further, the journal encourages articles from low- and middle-income countries, while also welcoming articles originated from South-South and South-North collaborations. All articles are expected to address a global agenda and include a strong implementation or policy component.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


