Thomas Gilder, Amanda Banaag, Cathaleen Madsen, Tracey Pèrez Koehlmoos
{"title":"Trends in Telehealth Care During the COVID-19 Pandemic for the Military Health System.","authors":"Thomas Gilder, Amanda Banaag, Cathaleen Madsen, Tracey Pèrez Koehlmoos","doi":"10.1089/tmr.2022.0042","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The COVID-19 pandemic generated a major shift from in-person to telehealth care in efforts to reduce the spread of infection. This study assesses the effects of COVID-19 on the provision of telehealth in the United States Military Health System (MHS), a universally-insured, nationally representative population of beneficiaries who may receive direct care (DC) at military facilities or in the private-sector care (PSC).</p><p><strong>Methods: </strong>Under a cross-sectional study design, we queried the MHS Data Repository for all telehealth services in the MHS from January 2019 to December 2021, using common procedure terminology code telehealth modifiers GT, GQ, and 95. Analyses were stratified by clinical, provider, and facility characteristics, and comparisons were made between telehealth rates before and during the COVID-19 period using a percent change.</p><p><strong>Results: </strong>Telehealth usage increased by 20-fold in 2020 versus 2019, whereas provider types shifted from predominantly physicians to advanced practice nurses and physician assistants. Patterns of task shifting were different between DC and PSC. Tele-mental health visits showed a 118% change in DC and -20% change in PSC, suggesting recapture of care to military facilities. Decreases in DC telehealth visits for metabolic, endocrine, and musculoskeletal disorders were not compensated by increases in PSC, suggesting care deferred, delivered by another modality, or sought outside the MHS.</p><p><strong>Conclusion: </strong>The increase in telehealth usage and behavioral health is in line with other published studies, whereas the shift in provider types aligns with MHS goals focused on increasing access through telehealth. More research is needed to answer questions of care deferral, which are relevant to national health care discussions.</p>","PeriodicalId":94218,"journal":{"name":"Telemedicine reports","volume":"4 1","pages":"147-155"},"PeriodicalIF":1.6000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10523401/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Telemedicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/tmr.2022.0042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: The COVID-19 pandemic generated a major shift from in-person to telehealth care in efforts to reduce the spread of infection. This study assesses the effects of COVID-19 on the provision of telehealth in the United States Military Health System (MHS), a universally-insured, nationally representative population of beneficiaries who may receive direct care (DC) at military facilities or in the private-sector care (PSC).
Methods: Under a cross-sectional study design, we queried the MHS Data Repository for all telehealth services in the MHS from January 2019 to December 2021, using common procedure terminology code telehealth modifiers GT, GQ, and 95. Analyses were stratified by clinical, provider, and facility characteristics, and comparisons were made between telehealth rates before and during the COVID-19 period using a percent change.
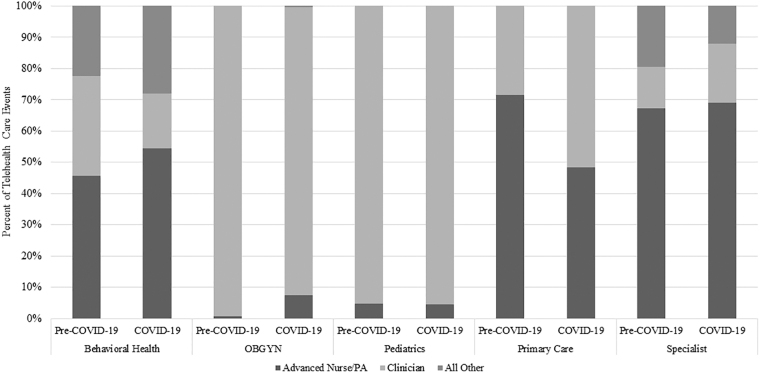
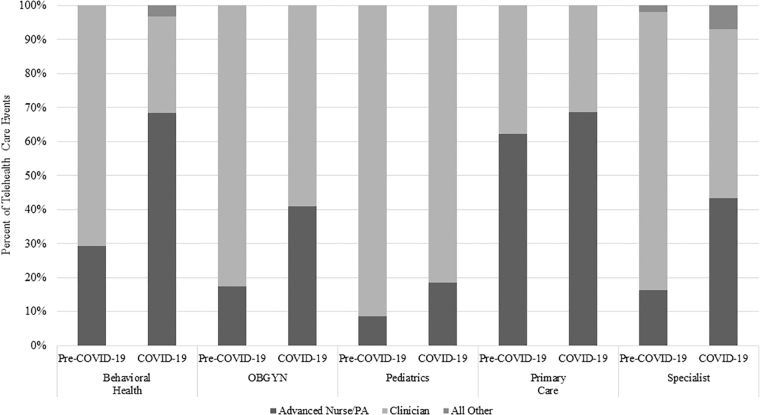
Results: Telehealth usage increased by 20-fold in 2020 versus 2019, whereas provider types shifted from predominantly physicians to advanced practice nurses and physician assistants. Patterns of task shifting were different between DC and PSC. Tele-mental health visits showed a 118% change in DC and -20% change in PSC, suggesting recapture of care to military facilities. Decreases in DC telehealth visits for metabolic, endocrine, and musculoskeletal disorders were not compensated by increases in PSC, suggesting care deferred, delivered by another modality, or sought outside the MHS.
Conclusion: The increase in telehealth usage and behavioral health is in line with other published studies, whereas the shift in provider types aligns with MHS goals focused on increasing access through telehealth. More research is needed to answer questions of care deferral, which are relevant to national health care discussions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


