A Pilot Standardized Simulation-Based Mechanical Ventilation Curriculum Targeting Pulmonary and Critical Care Medicine and Critical Care Medicine Fellows.
{"title":"A Pilot Standardized Simulation-Based Mechanical Ventilation Curriculum Targeting Pulmonary and Critical Care Medicine and Critical Care Medicine Fellows.","authors":"Amina Pervaiz, Asil Daoud, Abdulrazak Alchakaki, Shyam Ganti, Divya Venkat, Sarah Lee, Abdulghani Sankari","doi":"10.1055/s-0043-1773792","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> The mastery of mechanical ventilation (MV) management is challenging, as it requires the integration of physiological and technological knowledge with critical thinking. Our aim was to create a standardized curriculum with assessment tools based on evidence-based practices to identify the skill deficit and improve knowledge in MV management. <b>Methods</b> For 3 years, 3 hours of standardized curriculum for each first-year pulmonary critical care medicine (PCCM) and critical care medicine (CCM) fellows was integrated into the orientation (chronologically): (1) a baseline knowledge pretest; (2) a 1-hour one-on-one case-based simulation session with debriefing. A 34-item competency checklist was used to assess critically thinking and skills and guide the debriefing; (3) a 1-hour group didactic on respiratory mechanics and physiology; (4) a 45-minute hands-on session in small groups of one to three fellows for basic knobology, waveforms, and various modes of mechanical ventilators; (5) a 15-minute group bedside teaching of vented patients covering topics such as techniques to alleviate dyssynchrony and advanced ventilator modes; (6) a one-on-one simulation reassessment session; (7) a knowledge posttest. Fellows' performances at baseline, 1-month posttest, and end-of-first year post-test were compared. <b>Results</b> Fellows ( <i>n</i> = 24) demonstrated significant improvement at 1-month posttest in knowledge (54.2% ± 11.0 vs. 76.6 ± 11.7%, <i>p</i> < 0.001) and MV competency (40.7 ± 11.0% vs. 69.7 ± 9.3%, <i>p</i> < 0.001), compared with pretest. These improvements were retained at the end-of-year reassessments (knowledge 75.1 ± 14.5% and MV competency 85.5 ± 8.7%; <i>p</i> < 0.001). <b>Conclusion</b> Standardized simulation-based MV curriculum may improve the medical knowledge competency, and confidence of first-year PCCM and CCM fellows toward MV management before encountering actual ventilated patients.</p>","PeriodicalId":32889,"journal":{"name":"Avicenna Journal of Medicine","volume":"13 3","pages":"176-181"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10550363/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Avicenna Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1773792","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
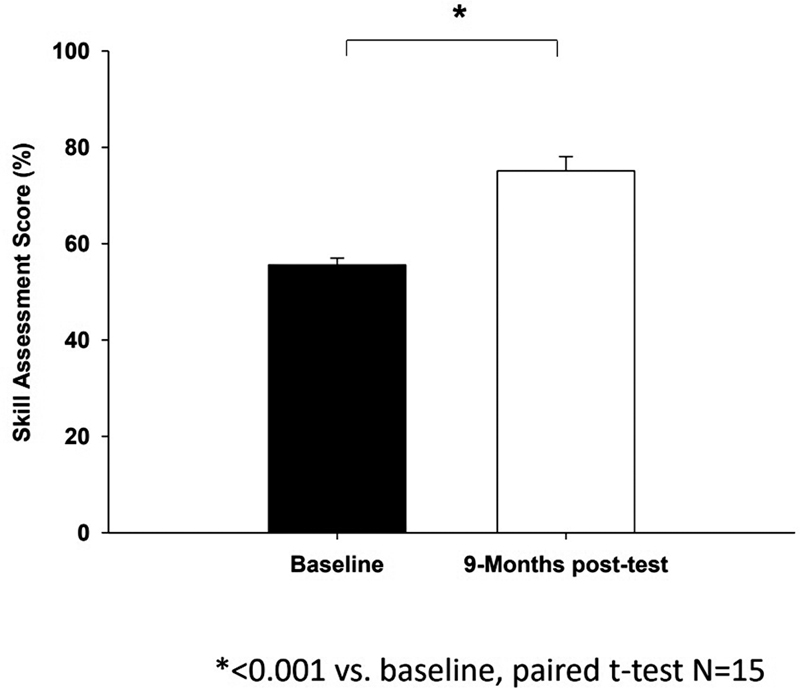
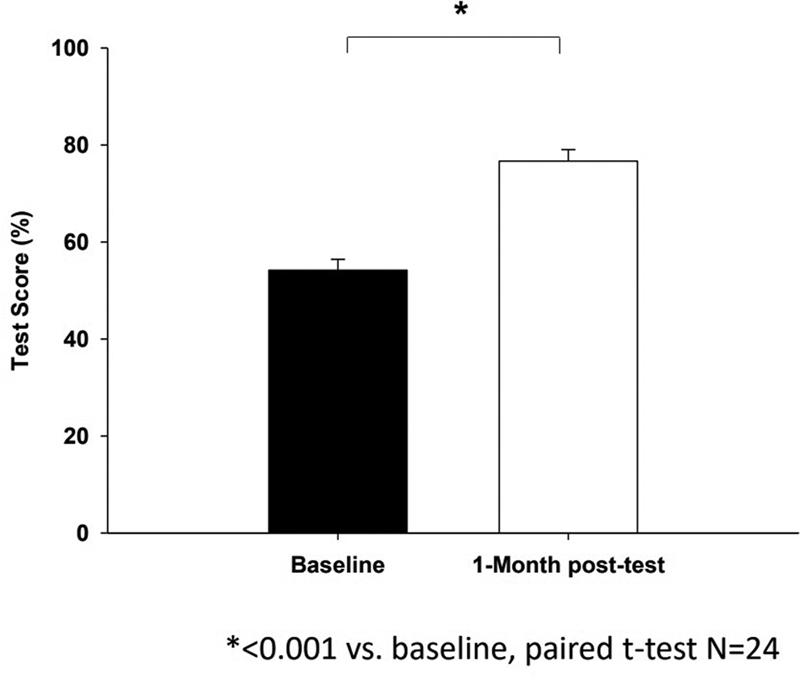
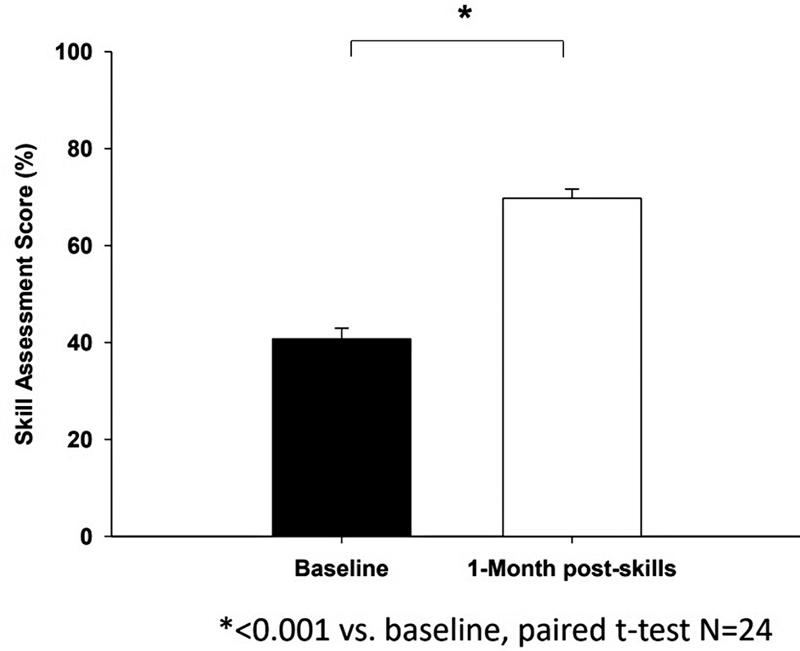
Introduction The mastery of mechanical ventilation (MV) management is challenging, as it requires the integration of physiological and technological knowledge with critical thinking. Our aim was to create a standardized curriculum with assessment tools based on evidence-based practices to identify the skill deficit and improve knowledge in MV management. Methods For 3 years, 3 hours of standardized curriculum for each first-year pulmonary critical care medicine (PCCM) and critical care medicine (CCM) fellows was integrated into the orientation (chronologically): (1) a baseline knowledge pretest; (2) a 1-hour one-on-one case-based simulation session with debriefing. A 34-item competency checklist was used to assess critically thinking and skills and guide the debriefing; (3) a 1-hour group didactic on respiratory mechanics and physiology; (4) a 45-minute hands-on session in small groups of one to three fellows for basic knobology, waveforms, and various modes of mechanical ventilators; (5) a 15-minute group bedside teaching of vented patients covering topics such as techniques to alleviate dyssynchrony and advanced ventilator modes; (6) a one-on-one simulation reassessment session; (7) a knowledge posttest. Fellows' performances at baseline, 1-month posttest, and end-of-first year post-test were compared. Results Fellows ( n = 24) demonstrated significant improvement at 1-month posttest in knowledge (54.2% ± 11.0 vs. 76.6 ± 11.7%, p < 0.001) and MV competency (40.7 ± 11.0% vs. 69.7 ± 9.3%, p < 0.001), compared with pretest. These improvements were retained at the end-of-year reassessments (knowledge 75.1 ± 14.5% and MV competency 85.5 ± 8.7%; p < 0.001). Conclusion Standardized simulation-based MV curriculum may improve the medical knowledge competency, and confidence of first-year PCCM and CCM fellows toward MV management before encountering actual ventilated patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


