Verena Broecker, Mats Brännström, Hans Bösmüller, Eva Sticová, Jana Malušková, Andres Chiesa-Vottero, Johan Mölne
{"title":"Reproducibility of Rejection Grading in Uterus Transplantation: A Multicenter Study.","authors":"Verena Broecker, Mats Brännström, Hans Bösmüller, Eva Sticová, Jana Malušková, Andres Chiesa-Vottero, Johan Mölne","doi":"10.1097/TXD.0000000000001535","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diagnosis of rejection after uterus transplantation is based on histopathological examination of ectocervical biopsies. Inflammation at the stromal-epithelial interface is the backbone of the histopathological classification proposed by our group in 2017. However, the reproducibility of this grading scheme has not been tested, and it is unclear whether it covers the full morphological spectrum of rejection.</p><p><strong>Methods: </strong>We present a multicenter study in which 5 pathologists from 4 uterus transplantation centers performed 2 rounds of grading on 145 and 48 cervical biopsies, respectively. Three of the centers provided biopsies. Additionally, the presence of perivascular stromal inflammation was recorded. During discussions after the first round, further histological lesions (venous endothelial inflammation and apoptosis) were identified for closer evaluation and added to the panel of lesions to score in the second round. All participants completed a questionnaire to explore current practices in handling and reporting uterus transplant biopsies.</p><p><strong>Results: </strong>Cervical biopsies were commonly performed in all centers to monitor rejection. Intraobserver reproducibility of rejection grading (performed by 1 rater) was excellent, whereas interobserver reproducibility was moderate and did not improve in the second round. Reproducibility of perivascular stromal inflammation was moderate but unsatisfactory for venous endothelial inflammation and apoptosis. All lesions were more frequent in, but not restricted to, biopsies with rejection patterns.</p><p><strong>Conclusions: </strong>Grading of rejection in cervical biopsies is reproducible and applicable to biopsies from different centers. Diagnosis of rejection may be improved by adding further histological lesions to the grading system; however, lesions require rigorous consensus definition.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"9 10","pages":"e1535"},"PeriodicalIF":1.9000,"publicationDate":"2023-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9d/89/txd-9-e1535.PMC10513355.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001535","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
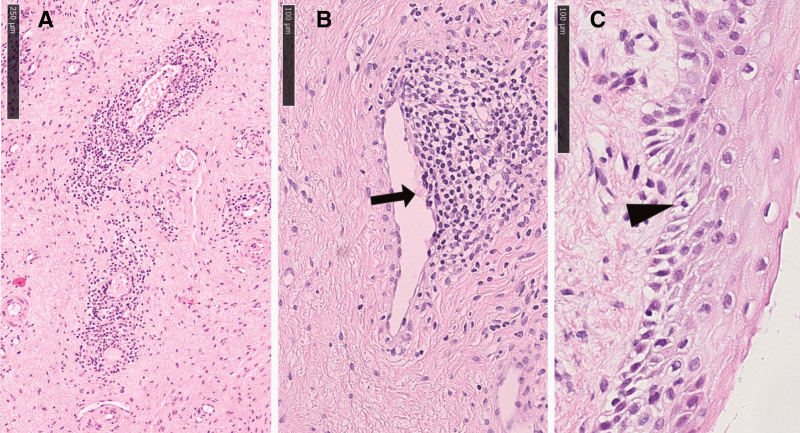
Background: Diagnosis of rejection after uterus transplantation is based on histopathological examination of ectocervical biopsies. Inflammation at the stromal-epithelial interface is the backbone of the histopathological classification proposed by our group in 2017. However, the reproducibility of this grading scheme has not been tested, and it is unclear whether it covers the full morphological spectrum of rejection.
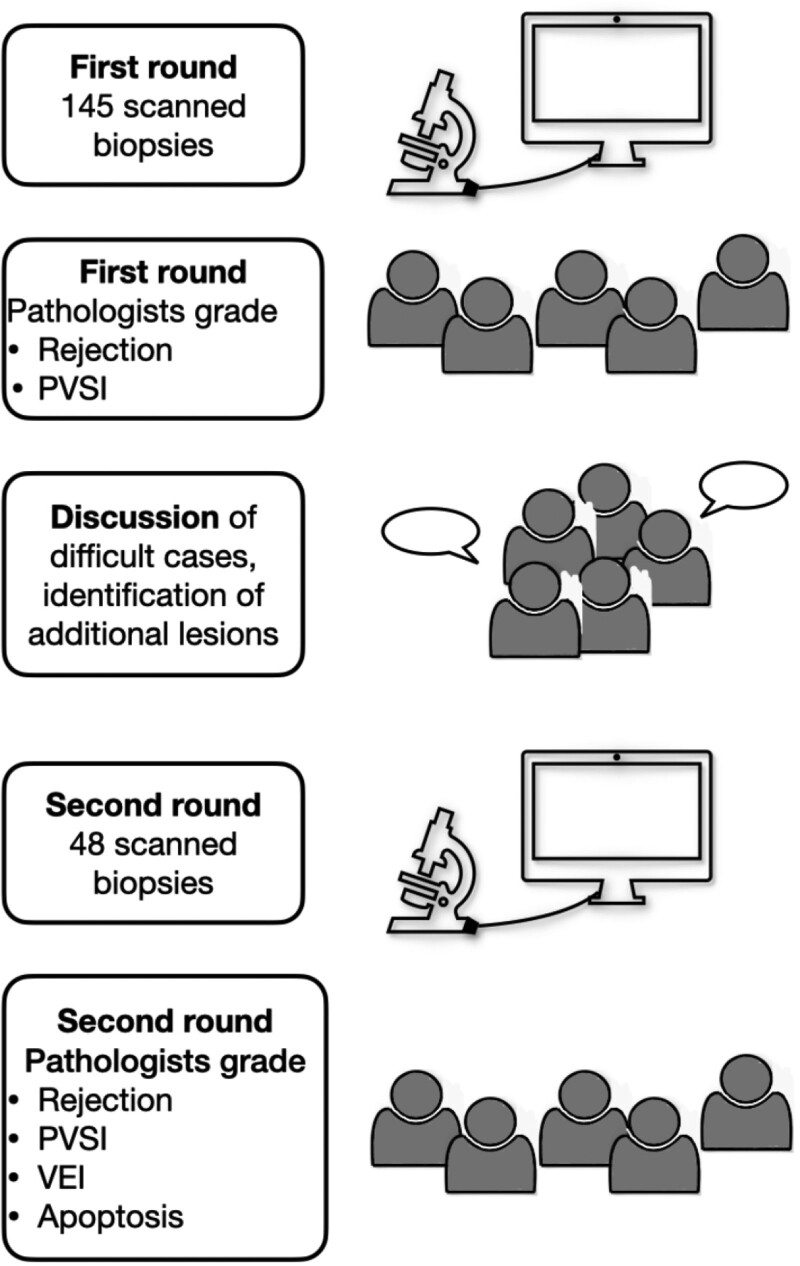
Methods: We present a multicenter study in which 5 pathologists from 4 uterus transplantation centers performed 2 rounds of grading on 145 and 48 cervical biopsies, respectively. Three of the centers provided biopsies. Additionally, the presence of perivascular stromal inflammation was recorded. During discussions after the first round, further histological lesions (venous endothelial inflammation and apoptosis) were identified for closer evaluation and added to the panel of lesions to score in the second round. All participants completed a questionnaire to explore current practices in handling and reporting uterus transplant biopsies.
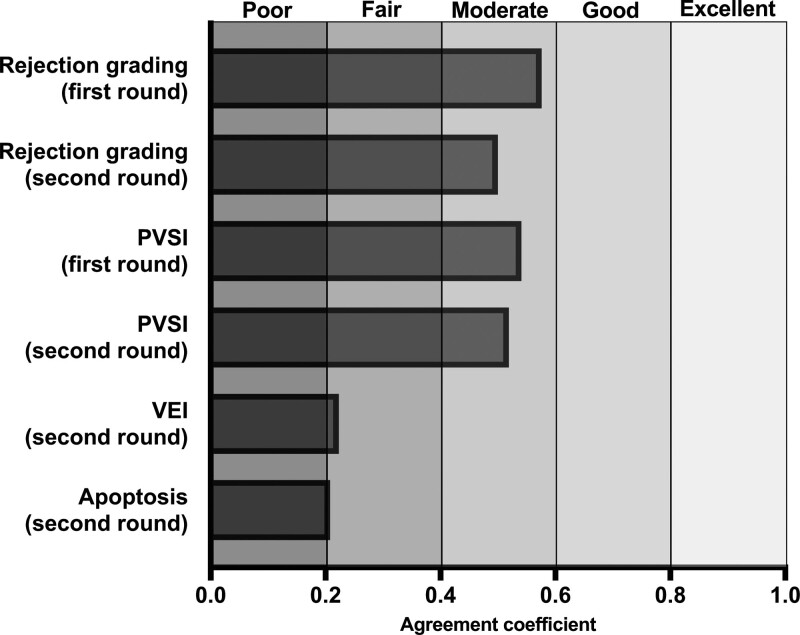
Results: Cervical biopsies were commonly performed in all centers to monitor rejection. Intraobserver reproducibility of rejection grading (performed by 1 rater) was excellent, whereas interobserver reproducibility was moderate and did not improve in the second round. Reproducibility of perivascular stromal inflammation was moderate but unsatisfactory for venous endothelial inflammation and apoptosis. All lesions were more frequent in, but not restricted to, biopsies with rejection patterns.
Conclusions: Grading of rejection in cervical biopsies is reproducible and applicable to biopsies from different centers. Diagnosis of rejection may be improved by adding further histological lesions to the grading system; however, lesions require rigorous consensus definition.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


