Julia C Dombrowski, Scott Halliday, Judith I Tsui, Deepa Rao, Kenneth Sherr, Meena S Ramchandani, Ramona Emerson, Mark Fleming, Teagan Wood, Lydia Chwastiak
{"title":"Adaptation of the collaborative care model to integrate behavioral health care into a low-barrier HIV clinic.","authors":"Julia C Dombrowski, Scott Halliday, Judith I Tsui, Deepa Rao, Kenneth Sherr, Meena S Ramchandani, Ramona Emerson, Mark Fleming, Teagan Wood, Lydia Chwastiak","doi":"10.1177/26334895231167105","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The collaborative care management (CoCM) model is an evidence-based intervention for integrating behavioral health care into nonpsychiatric settings. CoCM has been extensively studied in primary care clinics, but implementation in nonconventional clinics, such as those tailored to provide care for high-need, complex patients, has not been well described.</p><p><strong>Method: </strong>We adapted CoCM for a low-barrier HIV clinic that provides walk-in medical care for a patient population with high levels of mental illness, substance use, and housing instability. The Exploration, Preparation, Implementation, and Sustainment model guided implementation activities and support through the phases of implementing CoCM. The Framework for Reporting Adaptations and Modifications to Evidence-Based Interventions guided our documentation of adaptations to process-of-care elements and structural elements of CoCM. We used a multicomponent strategy to implement the adapted CoCM model. In this article, we describe our experience through the first 6 months of implementation.</p><p><strong>Results: </strong>The key contextual factors necessitating adaptation of the CoCM model were the clinic team structure, lack of scheduled appointments, high complexity of the patient population, and time constraints with competing priorities for patient care, all of which required substantial flexibility in the model. The process-of-care elements were adapted to improve the fit of the intervention with the context, but the core structural elements of CoCM were maintained.</p><p><strong>Conclusions: </strong>The CoCM model can be adapted for a setting that requires more flexibility than the usual primary care clinic while maintaining the core elements of the intervention.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"4 ","pages":"26334895231167105"},"PeriodicalIF":2.6000,"publicationDate":"2023-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/39/65/10.1177_26334895231167105.PMC10123894.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895231167105","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The collaborative care management (CoCM) model is an evidence-based intervention for integrating behavioral health care into nonpsychiatric settings. CoCM has been extensively studied in primary care clinics, but implementation in nonconventional clinics, such as those tailored to provide care for high-need, complex patients, has not been well described.
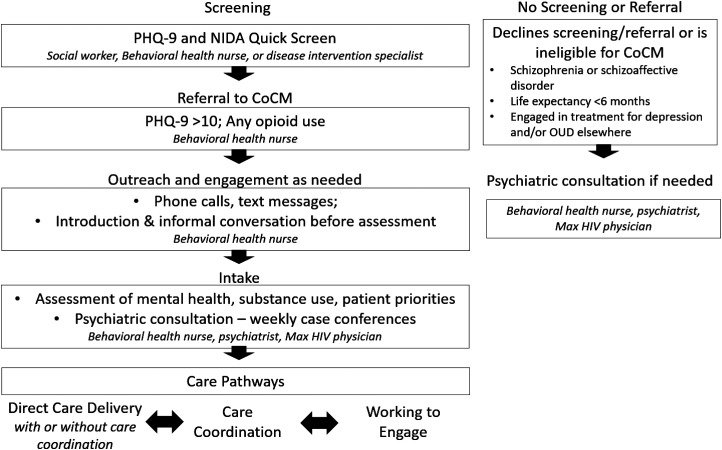
Method: We adapted CoCM for a low-barrier HIV clinic that provides walk-in medical care for a patient population with high levels of mental illness, substance use, and housing instability. The Exploration, Preparation, Implementation, and Sustainment model guided implementation activities and support through the phases of implementing CoCM. The Framework for Reporting Adaptations and Modifications to Evidence-Based Interventions guided our documentation of adaptations to process-of-care elements and structural elements of CoCM. We used a multicomponent strategy to implement the adapted CoCM model. In this article, we describe our experience through the first 6 months of implementation.
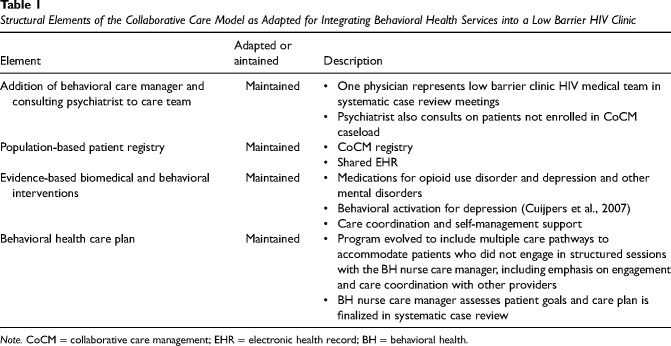
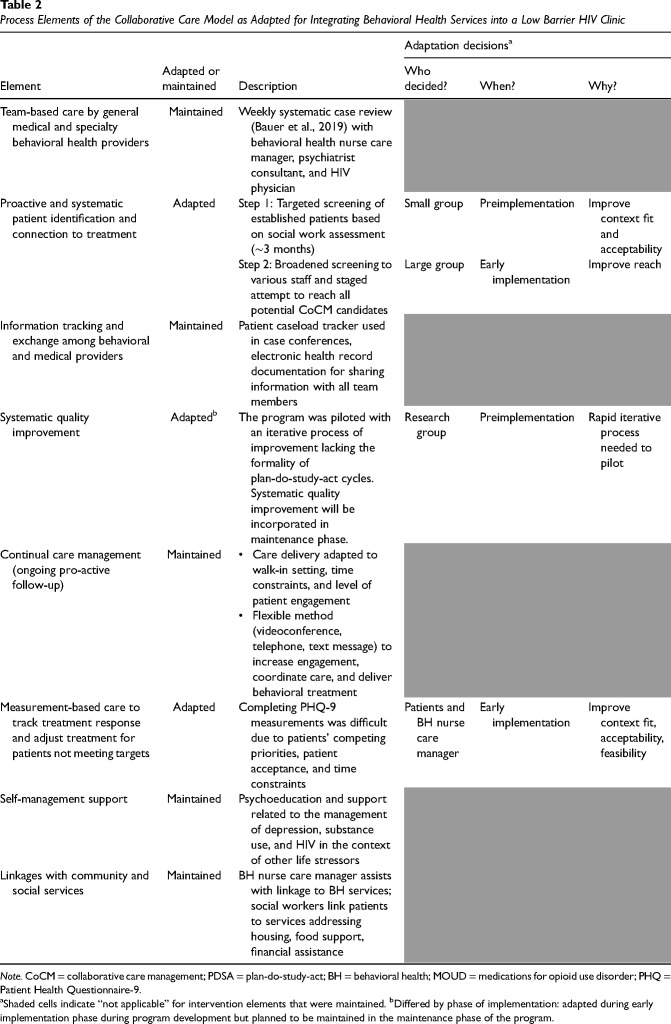
Results: The key contextual factors necessitating adaptation of the CoCM model were the clinic team structure, lack of scheduled appointments, high complexity of the patient population, and time constraints with competing priorities for patient care, all of which required substantial flexibility in the model. The process-of-care elements were adapted to improve the fit of the intervention with the context, but the core structural elements of CoCM were maintained.
Conclusions: The CoCM model can be adapted for a setting that requires more flexibility than the usual primary care clinic while maintaining the core elements of the intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


