Kaylen J Pfisterer, Raima Lohani, Elizabeth Janes, Denise Ng, Dan Wang, Denise Bryant-Lukosius, Ricardo Rendon, Alejandro Berlin, Jacqueline Bender, Ian Brown, Andrew Feifer, Geoffrey Gotto, Shumit Saha, Joseph A Cafazzo, Quynh Pham
{"title":"An Actionable Expert-System Algorithm to Support Nurse-Led Cancer Survivorship Care: Algorithm Development Study.","authors":"Kaylen J Pfisterer, Raima Lohani, Elizabeth Janes, Denise Ng, Dan Wang, Denise Bryant-Lukosius, Ricardo Rendon, Alejandro Berlin, Jacqueline Bender, Ian Brown, Andrew Feifer, Geoffrey Gotto, Shumit Saha, Joseph A Cafazzo, Quynh Pham","doi":"10.2196/44332","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Comprehensive models of survivorship care are necessary to improve access to and coordination of care. New models of care provide the opportunity to address the complexity of physical and psychosocial problems and long-term health needs experienced by patients following cancer treatment.</p><p><strong>Objective: </strong>This paper presents our expert-informed, rules-based survivorship algorithm to build a nurse-led model of survivorship care to support men living with prostate cancer (PCa). The algorithm is called No Evidence of Disease (Ned) and supports timelier decision-making, enhanced safety, and continuity of care.</p><p><strong>Methods: </strong>An initial rule set was developed and refined through working groups with clinical experts across Canada (eg, nurse experts, physician experts, and scientists; n=20), and patient partners (n=3). Algorithm priorities were defined through a multidisciplinary consensus meeting with clinical nurse specialists, nurse scientists, nurse practitioners, urologic oncologists, urologists, and radiation oncologists (n=17). The system was refined and validated using the nominal group technique.</p><p><strong>Results: </strong>Four levels of alert classification were established, initiated by responses on the Expanded Prostate Cancer Index Composite for Clinical Practice survey, and mediated by changes in minimal clinically important different alert thresholds, alert history, and clinical urgency with patient autonomy influencing clinical acuity. Patient autonomy was supported through tailored education as a first line of response, and alert escalation depending on a patient-initiated request for a nurse consultation.</p><p><strong>Conclusions: </strong>The Ned algorithm is positioned to facilitate PCa nurse-led care models with a high nurse-to-patient ratio. This novel expert-informed PCa survivorship care algorithm contains a defined escalation pathway for clinically urgent symptoms while honoring patient preference. Though further validation is required through a pragmatic trial, we anticipate the Ned algorithm will support timelier decision-making and enhance continuity of care through the automation of more frequent automated checkpoints, while empowering patients to self-manage their symptoms more effectively than standard care.</p><p><strong>International registered report identifier (irrid): </strong>RR2-10.1136/bmjopen-2020-045806.</p>","PeriodicalId":45538,"journal":{"name":"JMIR Cancer","volume":"9 ","pages":"e44332"},"PeriodicalIF":3.3000,"publicationDate":"2023-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10585445/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/44332","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Comprehensive models of survivorship care are necessary to improve access to and coordination of care. New models of care provide the opportunity to address the complexity of physical and psychosocial problems and long-term health needs experienced by patients following cancer treatment.
Objective: This paper presents our expert-informed, rules-based survivorship algorithm to build a nurse-led model of survivorship care to support men living with prostate cancer (PCa). The algorithm is called No Evidence of Disease (Ned) and supports timelier decision-making, enhanced safety, and continuity of care.
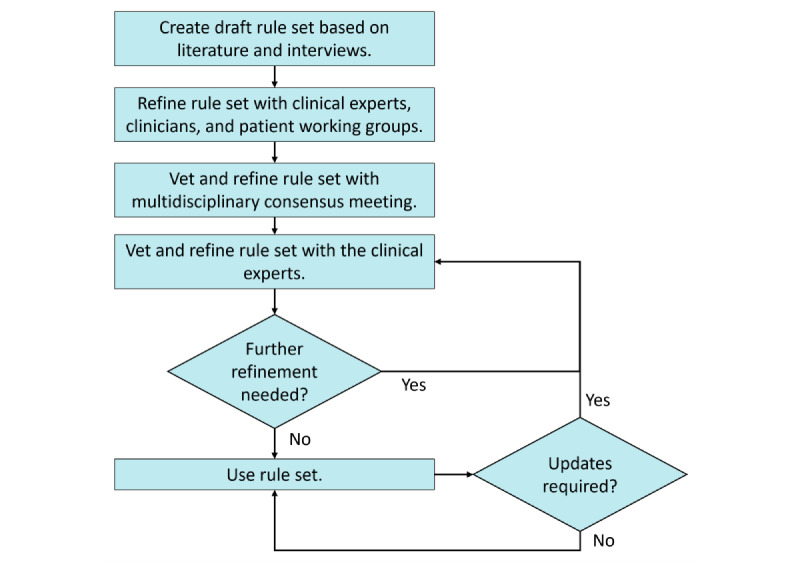
Methods: An initial rule set was developed and refined through working groups with clinical experts across Canada (eg, nurse experts, physician experts, and scientists; n=20), and patient partners (n=3). Algorithm priorities were defined through a multidisciplinary consensus meeting with clinical nurse specialists, nurse scientists, nurse practitioners, urologic oncologists, urologists, and radiation oncologists (n=17). The system was refined and validated using the nominal group technique.
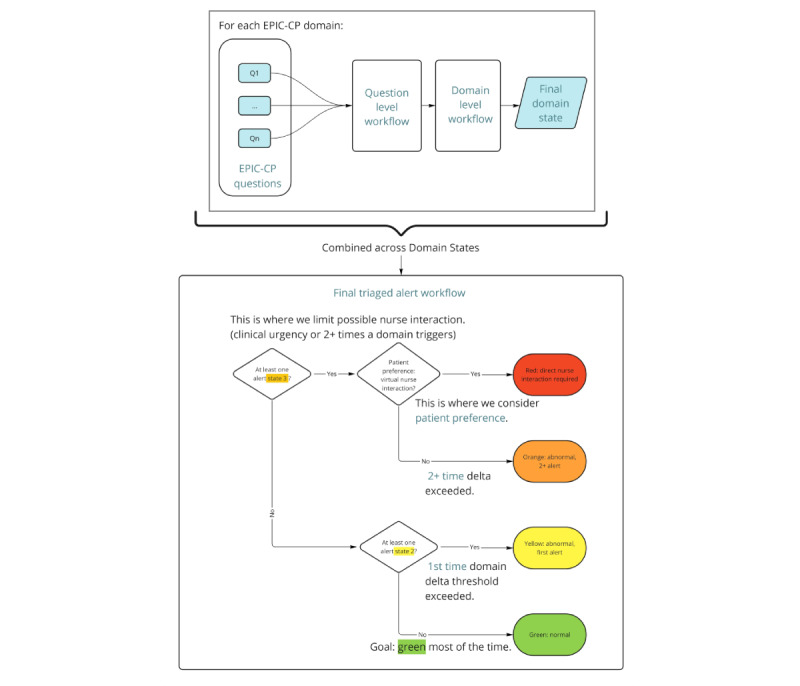
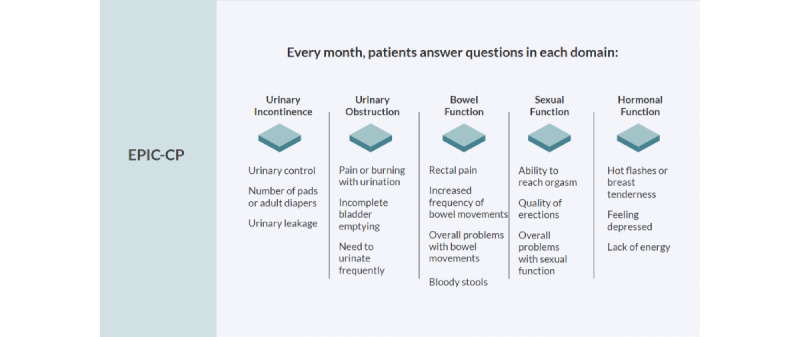
Results: Four levels of alert classification were established, initiated by responses on the Expanded Prostate Cancer Index Composite for Clinical Practice survey, and mediated by changes in minimal clinically important different alert thresholds, alert history, and clinical urgency with patient autonomy influencing clinical acuity. Patient autonomy was supported through tailored education as a first line of response, and alert escalation depending on a patient-initiated request for a nurse consultation.
Conclusions: The Ned algorithm is positioned to facilitate PCa nurse-led care models with a high nurse-to-patient ratio. This novel expert-informed PCa survivorship care algorithm contains a defined escalation pathway for clinically urgent symptoms while honoring patient preference. Though further validation is required through a pragmatic trial, we anticipate the Ned algorithm will support timelier decision-making and enhance continuity of care through the automation of more frequent automated checkpoints, while empowering patients to self-manage their symptoms more effectively than standard care.
International registered report identifier (irrid): RR2-10.1136/bmjopen-2020-045806.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


