{"title":"Ultrasonographic evaluation of the diaphragm in critically ill patients to predict invasive mechanical ventilation.","authors":"Karn Suttapanit, Supawit Wongkrasunt, Sorravit Savatmongkorngul, Praphaphorn Supatanakij","doi":"10.1186/s40560-023-00690-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diaphragm dysfunction is common in critically ill patients and associated with poorer outcomes. The function of the diaphragm can be evaluated at the bedside by measuring diaphragmatic excursion using ultrasonography. In this study, we investigated the ability of right-sided diaphragmatic excursion (RDE) to predict the need for invasive mechanical ventilation (IMV).</p><p><strong>Methods: </strong>Critically ill patients aged 18 years and older who presented to our emergency department between May 20, 2021 and May 19, 2022 and underwent measurement of RDE within 10 min of arrival were enrolled in this prospective study. The ability of RDE to predict the need for IMV was assessed by multivariable logistic regression and analysis of the area under the receiver-operating characteristic curve (AUROC).</p><p><strong>Results: </strong>A total of 314 patients were enrolled in the study; 113 (35.9%) of these patients required IMV. An increase of RDE value per each 0.1 cm was identified to be an independent predictor of IMV (adjusted odds ratio 0.08, 95% confidence interval [CI] 0.04-0.17, p < 0.001; AUROC 0.850, 95% CI 0.807-0.894). The RDE cutoff value was 1.2 cm (sensitivity 82.3%, 95% CI 74.0-88.8; specificity 78.1%, 95% CI 71.7-83.6). Time on a ventilator was significantly longer when the RDE was ≤ 1.2 cm (13 days [interquartile range 5, 27] versus 5 days [interquartile range 3, 8], p = 0.006).</p><p><strong>Conclusions: </strong>In this study, RDE had a good ability to predict the need for IMV in critically ill patients. The optimal RDE cutoff value was 1.2 cm. Its benefit in patient management requires further investigation.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"40"},"PeriodicalIF":3.8000,"publicationDate":"2023-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10507830/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00690-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Diaphragm dysfunction is common in critically ill patients and associated with poorer outcomes. The function of the diaphragm can be evaluated at the bedside by measuring diaphragmatic excursion using ultrasonography. In this study, we investigated the ability of right-sided diaphragmatic excursion (RDE) to predict the need for invasive mechanical ventilation (IMV).
Methods: Critically ill patients aged 18 years and older who presented to our emergency department between May 20, 2021 and May 19, 2022 and underwent measurement of RDE within 10 min of arrival were enrolled in this prospective study. The ability of RDE to predict the need for IMV was assessed by multivariable logistic regression and analysis of the area under the receiver-operating characteristic curve (AUROC).
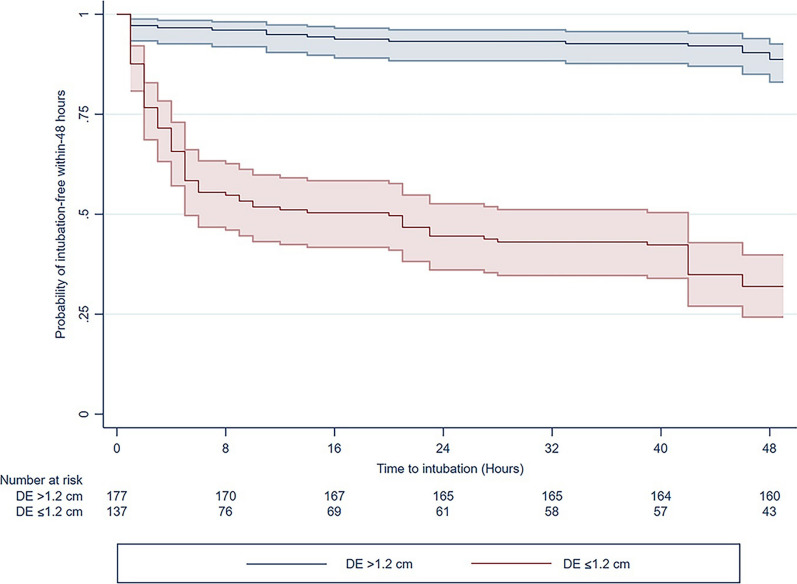
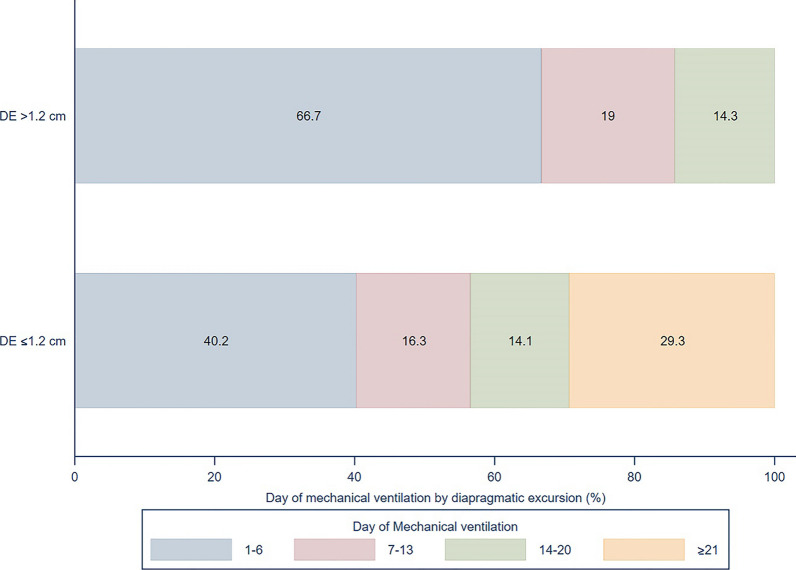
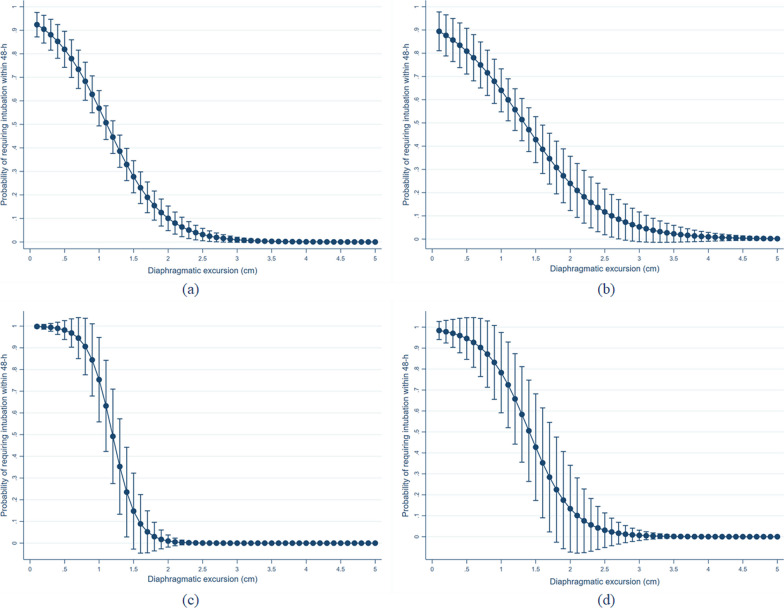
Results: A total of 314 patients were enrolled in the study; 113 (35.9%) of these patients required IMV. An increase of RDE value per each 0.1 cm was identified to be an independent predictor of IMV (adjusted odds ratio 0.08, 95% confidence interval [CI] 0.04-0.17, p < 0.001; AUROC 0.850, 95% CI 0.807-0.894). The RDE cutoff value was 1.2 cm (sensitivity 82.3%, 95% CI 74.0-88.8; specificity 78.1%, 95% CI 71.7-83.6). Time on a ventilator was significantly longer when the RDE was ≤ 1.2 cm (13 days [interquartile range 5, 27] versus 5 days [interquartile range 3, 8], p = 0.006).
Conclusions: In this study, RDE had a good ability to predict the need for IMV in critically ill patients. The optimal RDE cutoff value was 1.2 cm. Its benefit in patient management requires further investigation.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


