{"title":"Predictive factors for disease progression after salvage radiation therapy in biochemical recurrent patients treated by radical prostatectomy","authors":"Koichi Aikawa , Shoji Kimura , Fumihiko Urabe , Kosuke Iwatani , Kojiro Tashiro , Atsuhiko Ochi , Hirokazu Abe , Manabu Aoki , Takahiro Kimura","doi":"10.1016/j.prnil.2023.04.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Salvage radiation therapy (SRT) is standard treatment for patients after radical prostatectomy (RP). However, the optimal timing of SRT remains to be elucidated.</p></div><div><h3>Material and methods</h3><p>We retrospectively reviewed 133 prostate cancer (PCa) patients who underwent SRT for biochemical recurrence after RP. Disease progression was defined as repeated prostate-specific antigen (PSA) level more than 0.2 ng/mL, greater than the post-SRT nadir or radiographic progression. A receiver operating characteristic curve analysis was used to identify the optimal pre-SRT PSA level for predicting progression after SRT. Cox regression analyses were performed to elucidate the association between clinicopathologic characteristics and disease progression.</p></div><div><h3>Results</h3><p>Fifty-one PCa patients (38.4%) experienced disease progression after SRT. The optimal cutoff value of the pre-SRT PSA for predicting disease progression was 0.44 ng/mL. In multivariable analysis, pre-SRT PSA >0.44 ng/mL was a significant independent predictor of post-SRT disease progression [hazard ratio (HR): 2.02, <em>P</em> = 0.02]. Although the pre-SRT PSA >0.44 ng/mL did not maintain its independent association with disease progression in the multivariable analysis of patients with adverse pathology (HR: 1.63, <em>P</em> = 0.22), PSA within 4 weeks after RP as a continuous variable was significantly associated with disease progression (HR: 1.19, <em>P</em> = 0.04)</p></div><div><h3>Conclusions</h3><p>Our results highlight that in PCa patients who undergo RP, SRT should be performed before their PSA reaches 0.44 ng/mL. In patients with adverse pathology disease, a high PSA level within the 4 weeks after RP might identify those who are likely to have disease progression, and these patients might require systemic therapy.</p></div>","PeriodicalId":20845,"journal":{"name":"Prostate International","volume":"11 3","pages":"Pages 145-149"},"PeriodicalIF":2.6000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6f/6f/main.PMC10513901.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate International","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S228788822300017X","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Salvage radiation therapy (SRT) is standard treatment for patients after radical prostatectomy (RP). However, the optimal timing of SRT remains to be elucidated.
Material and methods
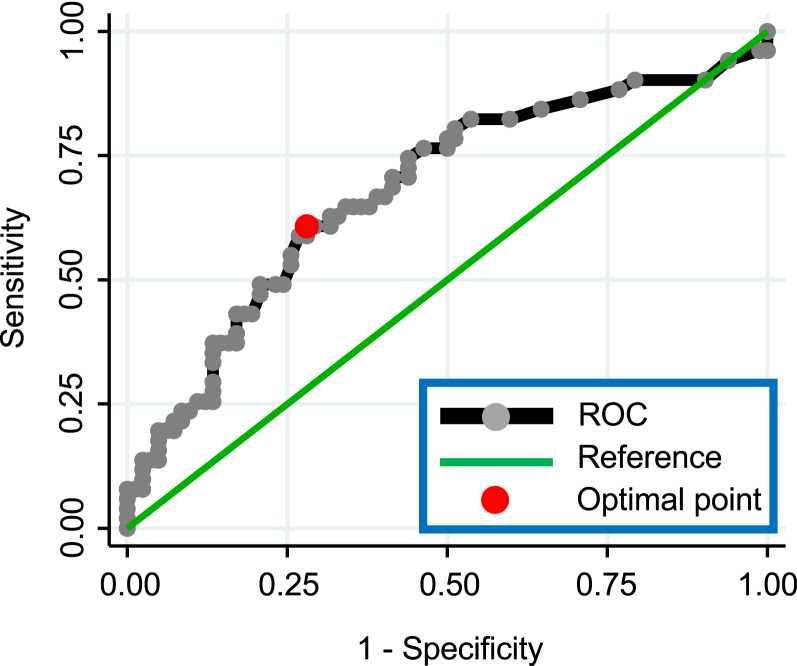
We retrospectively reviewed 133 prostate cancer (PCa) patients who underwent SRT for biochemical recurrence after RP. Disease progression was defined as repeated prostate-specific antigen (PSA) level more than 0.2 ng/mL, greater than the post-SRT nadir or radiographic progression. A receiver operating characteristic curve analysis was used to identify the optimal pre-SRT PSA level for predicting progression after SRT. Cox regression analyses were performed to elucidate the association between clinicopathologic characteristics and disease progression.
Results
Fifty-one PCa patients (38.4%) experienced disease progression after SRT. The optimal cutoff value of the pre-SRT PSA for predicting disease progression was 0.44 ng/mL. In multivariable analysis, pre-SRT PSA >0.44 ng/mL was a significant independent predictor of post-SRT disease progression [hazard ratio (HR): 2.02, P = 0.02]. Although the pre-SRT PSA >0.44 ng/mL did not maintain its independent association with disease progression in the multivariable analysis of patients with adverse pathology (HR: 1.63, P = 0.22), PSA within 4 weeks after RP as a continuous variable was significantly associated with disease progression (HR: 1.19, P = 0.04)
Conclusions
Our results highlight that in PCa patients who undergo RP, SRT should be performed before their PSA reaches 0.44 ng/mL. In patients with adverse pathology disease, a high PSA level within the 4 weeks after RP might identify those who are likely to have disease progression, and these patients might require systemic therapy.
期刊介绍:
Prostate International (Prostate Int, PI), the official English-language journal of Asian Pacific Prostate Society (APPS), is an international peer-reviewed academic journal dedicated to basic and clinical studies on prostate cancer, benign prostatic hyperplasia, prostatitis, and ...


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


