{"title":"Flexor Tendon Rupture Secondary to Gout.","authors":"Jeremy V Lynn, Amy L Strong, Kevin C Chung","doi":"10.1055/s-0043-1772756","DOIUrl":null,"url":null,"abstract":"<p><p>Extra-articular deposition of monosodium urate crystals is a widely recognized manifestation of gout. However, gouty infiltration of flexor tendons in the hand resulting in tendon rupture is exceedingly rare. This case report highlights a patient with gouty infiltration of flexor tendons in the right middle finger resulting in rupture of both the flexor digitorum profundus and flexor digitorum superficialis. Given the extent of gouty infiltration and need for pulley reconstruction, the patient was treated with two-stage flexor tendon reconstruction. Febuxostat was prescribed preoperatively to limit further deposition of monosodium urate crystals and continued postoperatively to maximize the potential for long-lasting results. Prednisone was prescribed between the first- and second-stage operations to prevent a gout flare while the silicone rod was in place. In summary, tendon rupture secondary to gouty infiltration is the most likely diagnosis in patients with a history of gout presenting with tendon insufficiency.</p>","PeriodicalId":47543,"journal":{"name":"Archives of Plastic Surgery-APS","volume":"50 5","pages":"492-495"},"PeriodicalIF":1.3000,"publicationDate":"2023-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10556320/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Plastic Surgery-APS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1772756","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
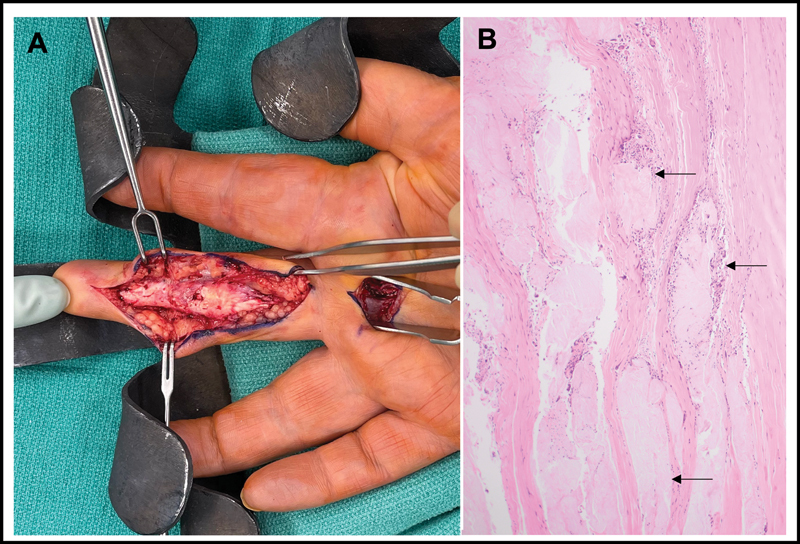
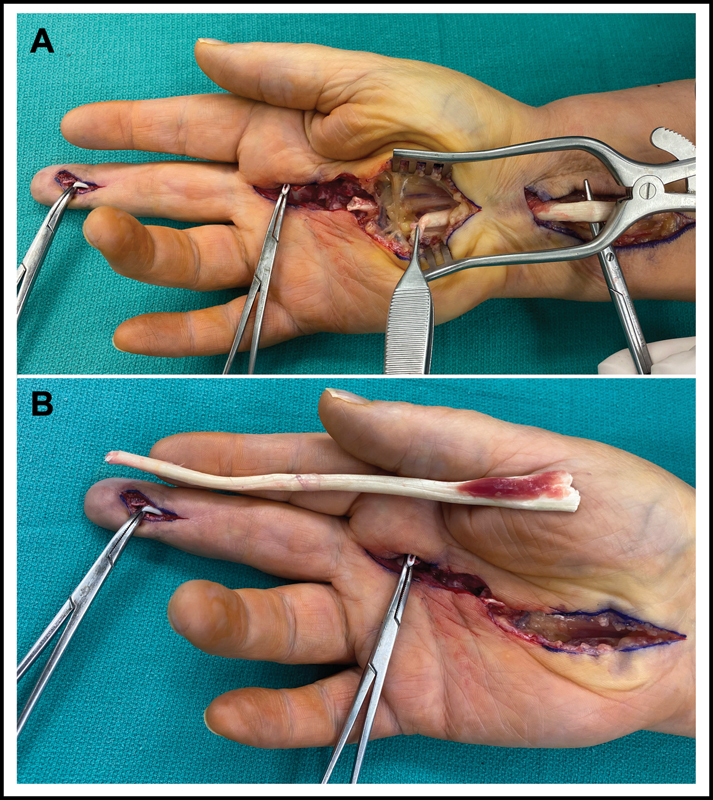
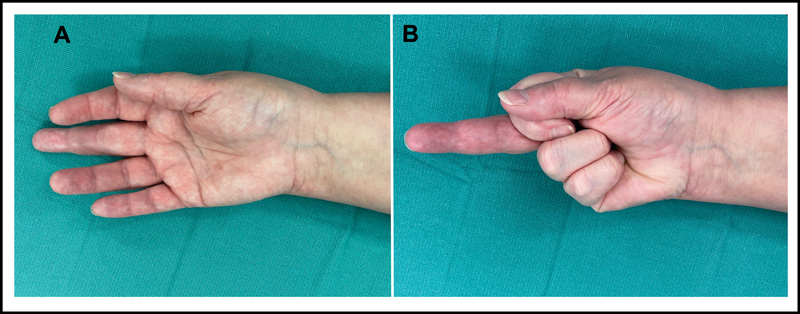
Extra-articular deposition of monosodium urate crystals is a widely recognized manifestation of gout. However, gouty infiltration of flexor tendons in the hand resulting in tendon rupture is exceedingly rare. This case report highlights a patient with gouty infiltration of flexor tendons in the right middle finger resulting in rupture of both the flexor digitorum profundus and flexor digitorum superficialis. Given the extent of gouty infiltration and need for pulley reconstruction, the patient was treated with two-stage flexor tendon reconstruction. Febuxostat was prescribed preoperatively to limit further deposition of monosodium urate crystals and continued postoperatively to maximize the potential for long-lasting results. Prednisone was prescribed between the first- and second-stage operations to prevent a gout flare while the silicone rod was in place. In summary, tendon rupture secondary to gouty infiltration is the most likely diagnosis in patients with a history of gout presenting with tendon insufficiency.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


