Cost-effectiveness analysis of abemaciclib with endocrine therapy (ET) versus ET alone for HR+, HER2-, node-positive, high-risk early breast cancer in Italy.
Alison Davie, Sory Traoré, Massimo Giovannitti, Giuseppe Pompilio, Mark Lambton, Esra Cakar, Anuja Chatterjee
{"title":"Cost-effectiveness analysis of abemaciclib with endocrine therapy (ET) versus ET alone for HR+, HER2-, node-positive, high-risk early breast cancer in Italy.","authors":"Alison Davie, Sory Traoré, Massimo Giovannitti, Giuseppe Pompilio, Mark Lambton, Esra Cakar, Anuja Chatterjee","doi":"10.33393/grhta.2023.2561","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Abemaciclib was recently approved by the European Medicines Agency in combination with adjuvant endocrine therapy (ET) for adult patients with hormone receptor positive (HR+), human epidermal growth factor receptor 2 negative (HER2-), node-positive early breast cancer (EBC) at high risk of recurrence.</p><p><strong>Objective: </strong>To evaluate the cost-effectiveness of abemaciclib plus ET vs. ET alone in patients with HR+, HER2-, node-positive EBC at high risk of disease recurrence, from the Italian healthcare system perspective.</p><p><strong>Methods: </strong>A cohort state transition model was developed with five states: invasive disease-free survival (IDFS), nonmetastatic recurrence, remission, metastatic recurrence, and death. The analysis had a time horizon of 30 years. Individual patient-level data from the monarchE trial (NCT03155997) were used to generate IDFS estimates. Resource use included drug acquisition/administration, best supportive care, terminal care, adverse events, hospitalization, post-progression therapy, and associated resource use in the metastatic disease health state. Health state utilities were derived from monarchE patient-level data and other sources, applying Italian tariffs where feasible.</p><p><strong>Results: </strong>The estimated total discounted costs (€39,249 vs. €16,806; difference: €22,443) and quality-adjusted life years (QALYs) (11.49 vs. 10.50; difference: 0.99) were higher for abemaciclib plus ET compared with ET alone. The incremental cost-effectiveness ratio was €22,651 per QALY gained. The likelihood of abemaciclib plus ET being cost-effective vs. ET alone was 99% at a willingness-to-pay threshold of €30,000 per QALY gained.</p><p><strong>Conclusion: </strong>Abemaciclib plus ET is a cost-effective treatment option vs. ET alone for those with HR+, HER2- node-positive EBC at high risk of recurrence in Italy.</p>","PeriodicalId":12627,"journal":{"name":"Global & Regional Health Technology Assessment","volume":"10 ","pages":"62-69"},"PeriodicalIF":0.5000,"publicationDate":"2023-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/22/ef/grhta-10-62.PMC10551672.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global & Regional Health Technology Assessment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.33393/grhta.2023.2561","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Abemaciclib was recently approved by the European Medicines Agency in combination with adjuvant endocrine therapy (ET) for adult patients with hormone receptor positive (HR+), human epidermal growth factor receptor 2 negative (HER2-), node-positive early breast cancer (EBC) at high risk of recurrence.
Objective: To evaluate the cost-effectiveness of abemaciclib plus ET vs. ET alone in patients with HR+, HER2-, node-positive EBC at high risk of disease recurrence, from the Italian healthcare system perspective.
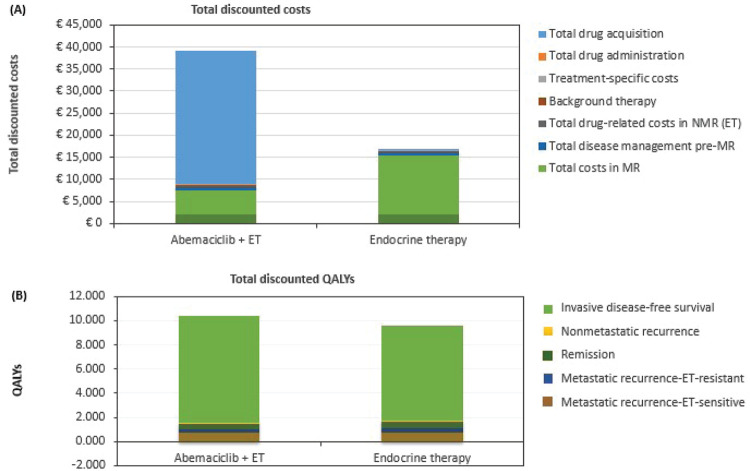
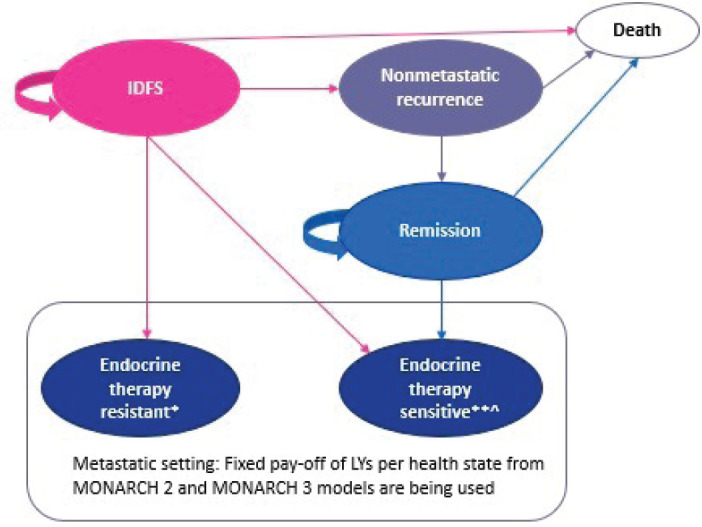
Methods: A cohort state transition model was developed with five states: invasive disease-free survival (IDFS), nonmetastatic recurrence, remission, metastatic recurrence, and death. The analysis had a time horizon of 30 years. Individual patient-level data from the monarchE trial (NCT03155997) were used to generate IDFS estimates. Resource use included drug acquisition/administration, best supportive care, terminal care, adverse events, hospitalization, post-progression therapy, and associated resource use in the metastatic disease health state. Health state utilities were derived from monarchE patient-level data and other sources, applying Italian tariffs where feasible.
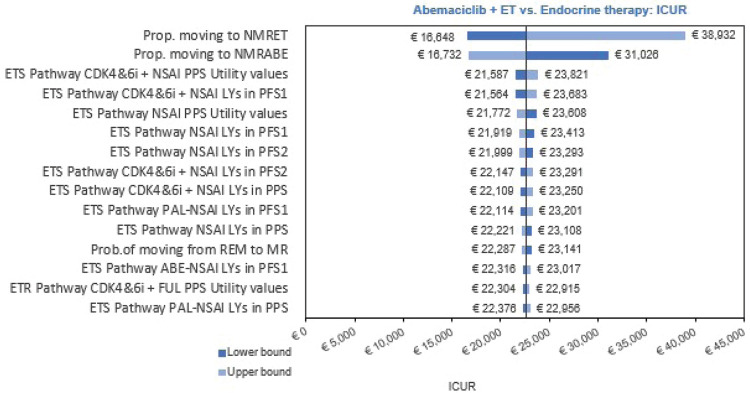
Results: The estimated total discounted costs (€39,249 vs. €16,806; difference: €22,443) and quality-adjusted life years (QALYs) (11.49 vs. 10.50; difference: 0.99) were higher for abemaciclib plus ET compared with ET alone. The incremental cost-effectiveness ratio was €22,651 per QALY gained. The likelihood of abemaciclib plus ET being cost-effective vs. ET alone was 99% at a willingness-to-pay threshold of €30,000 per QALY gained.
Conclusion: Abemaciclib plus ET is a cost-effective treatment option vs. ET alone for those with HR+, HER2- node-positive EBC at high risk of recurrence in Italy.
期刊介绍:
Global & Regional Health Technology Assessment (GRHTA) is a peer-reviewed, open access journal which aims to promote health technology assessment and economic evaluation, enabling choices among alternative therapeutical paths or procedures with different clinical and economic outcomes. GRHTA is a unique journal having three different editorial boards who focus on their respective geographical expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


