{"title":"Statin-Induced Necrotizing Autoimmune Myositis.","authors":"Yonatan Akivis, Meenakshi Kurup, Sabu John","doi":"10.14740/jmc4010","DOIUrl":null,"url":null,"abstract":"<p><p>Statins are the most frequently prescribed medications for primary and secondary prevention of atherosclerotic cardiovascular disease (ASCVD). The United States Preventative Services Task Force recommends that clinicians selectively offer a statin for the primary prevention of ASCVD for adults aged 40 - 75 years with one or more cardiovascular disease risk factors and an estimated 10-year risk of a cardiovascular event of 10% or greater. Despite their ubiquity, it is estimated that approximately 6-10% of patients remain intolerant due to muscle aches. Here, we present a case of a 71-year-old female that was taking atorvastatin for a year and presented to the emergency room with proximal muscle aches and weakness. Laboratory values were significant for an elevated creatinine kinase of 4,166 U/L (reference range, 20 - 180). Her magnetic resonance imaging was significant for edema in bilateral lower extremity proximal muscles. Serology revealed a high anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase antibody, confirming the diagnosis of statin-induced necrotizing autoimmune myositis. A muscle biopsy of the right vastus lateralis revealed necrotic muscle fibers. During her hospital course, she was treated with intravenous methylprednisolone, mycophenolate mofetil, and tacrolimus. Her symptoms gradually improved, and she was discharged after 14 days with a rheumatology follow-up. This is an exceedingly rare complication of statin use and has only recently received increasing attention. Here we present our experience with this disease.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"13 10","pages":"513-516"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d8/c2/jmc-13-513.PMC9635764.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
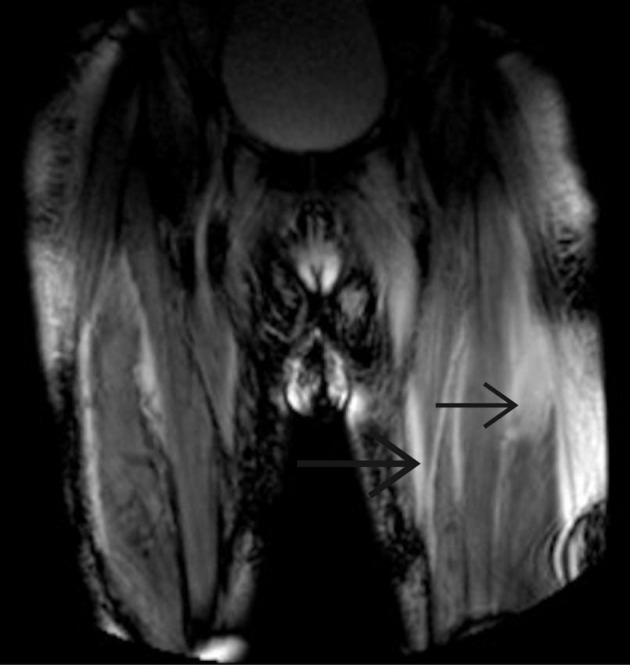
Statins are the most frequently prescribed medications for primary and secondary prevention of atherosclerotic cardiovascular disease (ASCVD). The United States Preventative Services Task Force recommends that clinicians selectively offer a statin for the primary prevention of ASCVD for adults aged 40 - 75 years with one or more cardiovascular disease risk factors and an estimated 10-year risk of a cardiovascular event of 10% or greater. Despite their ubiquity, it is estimated that approximately 6-10% of patients remain intolerant due to muscle aches. Here, we present a case of a 71-year-old female that was taking atorvastatin for a year and presented to the emergency room with proximal muscle aches and weakness. Laboratory values were significant for an elevated creatinine kinase of 4,166 U/L (reference range, 20 - 180). Her magnetic resonance imaging was significant for edema in bilateral lower extremity proximal muscles. Serology revealed a high anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase antibody, confirming the diagnosis of statin-induced necrotizing autoimmune myositis. A muscle biopsy of the right vastus lateralis revealed necrotic muscle fibers. During her hospital course, she was treated with intravenous methylprednisolone, mycophenolate mofetil, and tacrolimus. Her symptoms gradually improved, and she was discharged after 14 days with a rheumatology follow-up. This is an exceedingly rare complication of statin use and has only recently received increasing attention. Here we present our experience with this disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


