Thrombophlebitis Migrans As the Prodrome of Adult T-Cell Leukemia-Lymphoma.
IF 1.5
4区 医学
Q3 DERMATOLOGY
引用次数: 0
Abstract
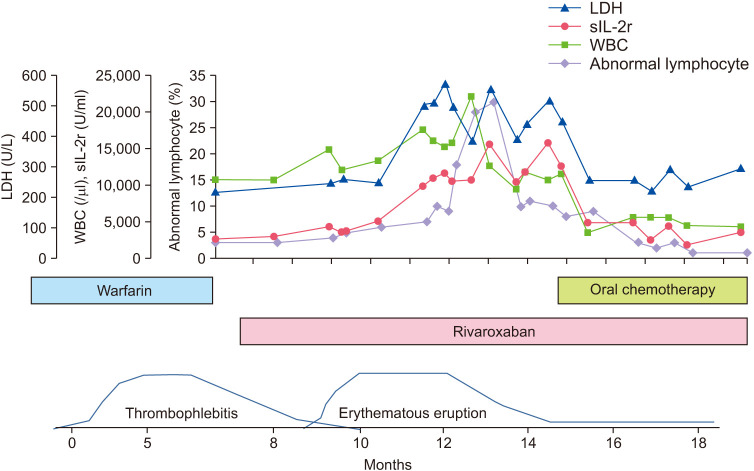
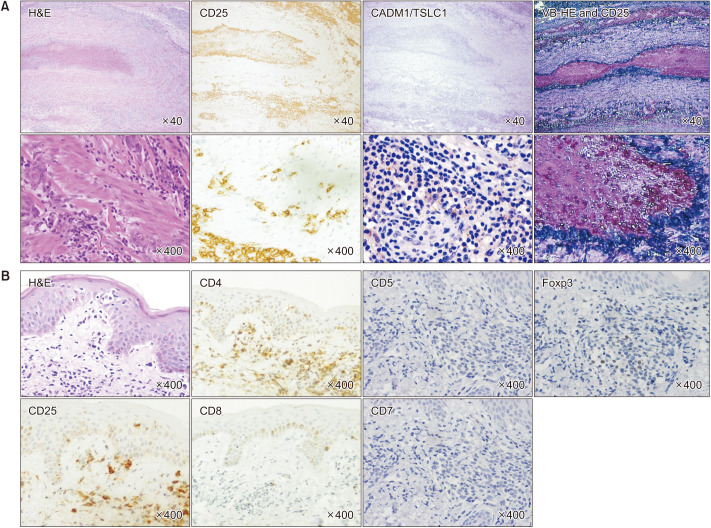
Dear Editor: A 70s male smoker (20 cigarettes/day for 23 years) and human T-lymphotropic virus type 1 (HTLV-1) carrier, developed painful nodular erythema in both wrist joints, the lower extremities and in the testes, each of which underwent 1-month cycles of repeating spontaneous regression and recurrence without any medications. He presented to our hospital 4 months after the initial symptom appeared (data not shown). A biopsy of a representative lesion revealed thrombosis in the deep dermis without leukocytoclastic vasculitis (Fig. 1A). There was neither fibrinoid necrosis nor a granulomatous lesion. A diagnosis of thrombophlebitis migrans was made. The white blood cell count (9,580/μl; normal range 2,950~ 8,970/μl) was increased, with 3% abnormal lymphocytes. Southern blot analysis of peripheral blood revealed an HTLV1 provirus DNA monoclonal band. Serum levels of C-reactive protein (3.57 mg/dl; normal range <0.21 mg/dl), soluble interleukin-2 receptor (2,498 U/ml; normal range 145~519 U/ml) and immunoglobulin A (459 mg/dl; normal range 110~410 mg/dl) also were increased. Because of a history of atrial fibrillation he was taking warfarin, therefore, prothrombin time international-normalized ratio was moderately prolonged (2.13; normal range 0.9~1.1). Protein C, protein S, antithrombin III, and fibrin/fibrinogen degradation products were within normal limits under transient heparinization after interruption of warfarin. Lupus anticoagulant, anticardiolipin antibodies, rapid plasma reagin test, treponema pallidum hemagglutination test and several tumor markers (i.e., squamous cell carcinoma antigen, α-fetoprotein, carcinoembryonic antigen, prostate specific antigen, carbohydrate antigen 19-9) were all negative or within the normal range. Computed tomography (CT) of the total body except for extremities and CT angiography revealed neither a solid mass nor vessel stenosis. His human leukocyte antigen (HLA) alleles were HLA-A*24, A*31, B*07, B*35, which are not associated with Behçet disease. He was diagnosed as smoldering adult T-cell leukemia-lymphoma (ATL) according to the Shimoyama criteria at the initial diagnosis. The clinical course of the present case is described in Fig. 2. Oral administration of rivaroxaban was started instead of warfarin and, thereafter, thrombophlebitis resolved with no further recurrence. Around the disappearance of thrombophlebitis, erythematous maculopapular eruptions were noted to be scattered over the entire body (data not shown); this was followed by HTLV-1-associated arthropathy, and lung disease. Findings of histological findings including immunohistochemical analysis of erythematous areas were consistent with those of ATL (Fig. 1B). His disease status changed to intermediate types between Received July 6, 2020 Revised November 10, 2020 Accepted December 19, 2020
移动性血栓性静脉炎是成人t细胞白血病-淋巴瘤的前驱症状。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Annals of Dermatology
医学-皮肤病学
CiteScore
1.60
自引率
6.20%
发文量
77
审稿时长
6-12 weeks
期刊介绍:
Annals of Dermatology (Ann Dermatol) is the official peer-reviewed publication of the Korean Dermatological Association and the Korean Society for Investigative Dermatology. Since 1989, Ann Dermatol has contributed as a platform for communicating the latest research outcome and recent trend of dermatology in Korea and all over the world.
Ann Dermatol seeks for ameliorated understanding of skin and skin-related disease for clinicians and researchers. Ann Dermatol deals with diverse skin-related topics from laboratory investigations to clinical outcomes and invites review articles, original articles, case reports, brief reports and items of correspondence. Ann Dermatol is interested in contributions from all countries in which good and advanced research is carried out. Ann Dermatol willingly recruits well-organized and significant manuscripts with proper scope throughout the world.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


