{"title":"Urinary stone in a 12-year-old adolescent with new-onset type 1 diabetes and diabetic ketoacidosis.","authors":"Kikumi Ushijima-Fuchino, Yuko Koga, Satoko Umino, Junko Nishioka, Junichiro Araki, Shuichi Yatsuga, Yushiro Yamashita","doi":"10.1297/cpe.2021-0069","DOIUrl":null,"url":null,"abstract":"<p><p>Dehydration and acidosis increase the risk for urinary stone formation. Urinary stones have been reported in three pediatric cases of diabetic ketoacidosis (DKA). A 24-h urine collection was performed for two of the three children. One patient had high urine sodium levels, while the other had low urine citrate excretion. We report the case of a 12-yr-old adolescent boy with urinary stones, new-onset type 1 diabetes mellitus (T1D), and DKA, excluding other metabolic disorders. After DKA was diagnosed, the patient received a 0.9% saline bolus and continuous insulin infusion. Hyperglycemia and ketoacidosis were well-controlled on the third day after admission. However, the patient developed abdominal pain radiating to the back. Urinary stones were suspected, and a urinalysis was performed. The patient's urine revealed significant elevation in red blood cells and calcium oxalate crystals. Computed tomography revealed a high-density left ureteric mass, suggestive of a urinary stone. Although both the previously reported pediatric cases involved metabolic diseases, additional tests in this patient excluded metabolic diseases other than T1D. DKA may be related to the formation of calcium oxalate crystals owing to dehydration and acidosis. Therefore, physicians should consider urinary stone formation in DKA patients.</p>","PeriodicalId":10678,"journal":{"name":"Clinical Pediatric Endocrinology","volume":"31 3","pages":"199-204"},"PeriodicalIF":1.2000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d4/95/cpe-31-199.PMC9297177.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1297/cpe.2021-0069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/8 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
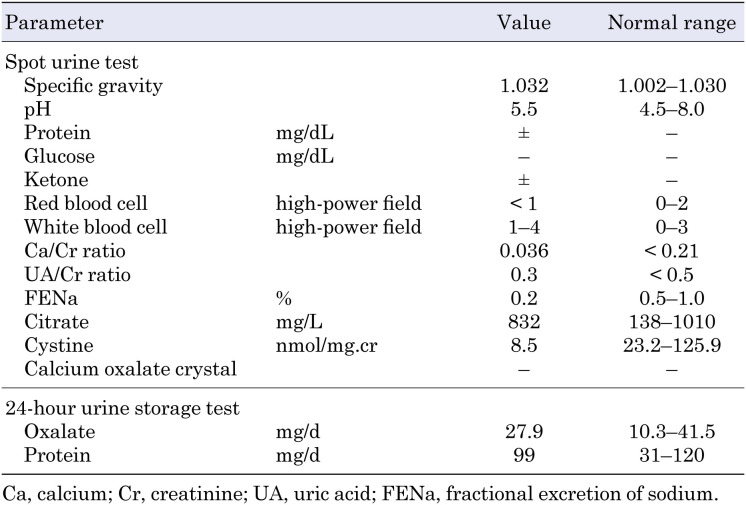
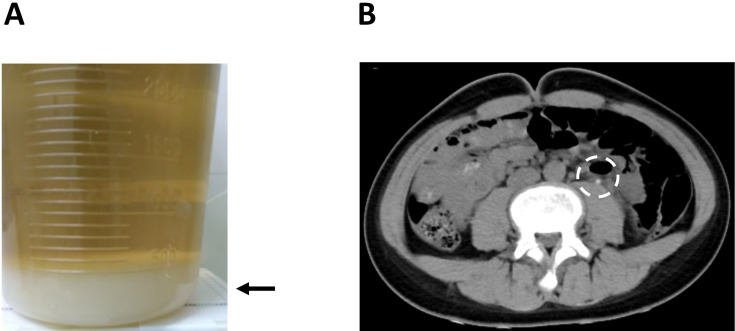
Dehydration and acidosis increase the risk for urinary stone formation. Urinary stones have been reported in three pediatric cases of diabetic ketoacidosis (DKA). A 24-h urine collection was performed for two of the three children. One patient had high urine sodium levels, while the other had low urine citrate excretion. We report the case of a 12-yr-old adolescent boy with urinary stones, new-onset type 1 diabetes mellitus (T1D), and DKA, excluding other metabolic disorders. After DKA was diagnosed, the patient received a 0.9% saline bolus and continuous insulin infusion. Hyperglycemia and ketoacidosis were well-controlled on the third day after admission. However, the patient developed abdominal pain radiating to the back. Urinary stones were suspected, and a urinalysis was performed. The patient's urine revealed significant elevation in red blood cells and calcium oxalate crystals. Computed tomography revealed a high-density left ureteric mass, suggestive of a urinary stone. Although both the previously reported pediatric cases involved metabolic diseases, additional tests in this patient excluded metabolic diseases other than T1D. DKA may be related to the formation of calcium oxalate crystals owing to dehydration and acidosis. Therefore, physicians should consider urinary stone formation in DKA patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


