A Case Report of Pericardial Effusion with False-Positive Mesothelioma and Adenocarcinoma Markers as the Initial Presentation of Systemic Lupus Erythematous.
{"title":"A Case Report of Pericardial Effusion with False-Positive Mesothelioma and Adenocarcinoma Markers as the Initial Presentation of Systemic Lupus Erythematous.","authors":"Gita Bhattacharya, Pritha P Gupta","doi":"10.1155/2022/8081055","DOIUrl":null,"url":null,"abstract":"<p><p>Pericardial effusion or the accumulation of fluid in the pericardial sac, can result from infectious, malignant, or autoimmune processes such as systemic lupus erythematous (SLE). However, pericardial effusion is infrequently the first presentation of SLE. Here, we describe the case of a 54-year-old African American woman who presented with hypertensive emergency and was found to have pericardial effusion on echocardiogram. Her hypertensive symptoms resolved with medical management and a work up were positive for serum markers of SLE and mesothelioma cell markers (calretinin, CK 5/6) and adenocarcinoma marker MOC31 in the pericardial fluid. Her effusion ultimately improved on high-dose steroid therapy and has not recurred in one year. Given normal pleura and pericardium on computed tomography (CT) imaging and long-term clinical improvement in SLE therapy, we hypothesize that she had false-positive mesothelioma markers in the setting of SLE.</p>","PeriodicalId":9622,"journal":{"name":"Case Reports in Rheumatology","volume":" ","pages":"8081055"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9649300/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/8081055","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
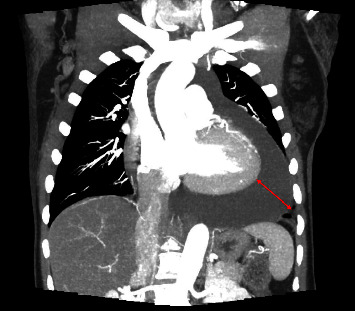
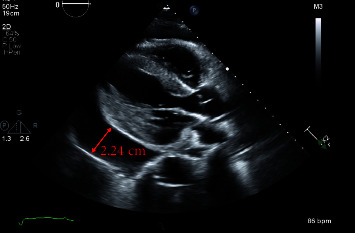
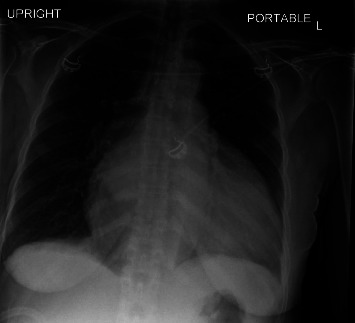
Pericardial effusion or the accumulation of fluid in the pericardial sac, can result from infectious, malignant, or autoimmune processes such as systemic lupus erythematous (SLE). However, pericardial effusion is infrequently the first presentation of SLE. Here, we describe the case of a 54-year-old African American woman who presented with hypertensive emergency and was found to have pericardial effusion on echocardiogram. Her hypertensive symptoms resolved with medical management and a work up were positive for serum markers of SLE and mesothelioma cell markers (calretinin, CK 5/6) and adenocarcinoma marker MOC31 in the pericardial fluid. Her effusion ultimately improved on high-dose steroid therapy and has not recurred in one year. Given normal pleura and pericardium on computed tomography (CT) imaging and long-term clinical improvement in SLE therapy, we hypothesize that she had false-positive mesothelioma markers in the setting of SLE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


