Michelle Howard, Abe Hafid, Colleen Webber, Sarina R Isenberg, Ana Gayowsky, Aaron Jones, Mary Scott, Amy T Hsu, Katrin Conen, James Downar, Doug Manuel, Peter Tanuseputro
{"title":"Continuity of physician care over the last year of life for different cause-of-death categories: a retrospective population-based study.","authors":"Michelle Howard, Abe Hafid, Colleen Webber, Sarina R Isenberg, Ana Gayowsky, Aaron Jones, Mary Scott, Amy T Hsu, Katrin Conen, James Downar, Doug Manuel, Peter Tanuseputro","doi":"10.9778/cmajo.20210294","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The mix of care provided by family physicians, specialists and palliative care physicians can vary by the illnesses leading to death, which may result in disruptions of continuity of care at the end of life. We measured continuity of outpatient physician care in the last year of life across differing causes of death and assessed factors associated with higher continuity.</p><p><strong>Methods: </strong>We conducted a retrospective descriptive study of adults who died in Ontario between 2013 and 2018, using linked provincial health administrative data. We calculated 3 measures of continuity (usual provider, Bice-Boxerman and sequential continuity), which range from 0 to 1, from outpatient physician visits over the last year of life for terminal illness, organ failure, frailty, sudden death and other causes of death. We used multivariable logistic regression models to evaluate associations between characteristics and a continuity score of 0.5 or greater.</p><p><strong>Results: </strong>Among the 417 628 decedents, we found that mean usual provider, Bice-Boxerman and sequential continuity indices were 0.37, 0.30 and 0.37, respectively, with continuity being the lowest for those with terminal illness (0.27, 0.23 and 0.33, respectively). Higher number of comorbidities, higher neighbourhood income quintile and all non-sudden death categories were associated with lower continuity.</p><p><strong>Interpretation: </strong>We found that continuity of physician care in the last year of life was low, especially in those with cancer. Further research is needed to validate measures of continuity against end-of-life health care outcomes.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":" ","pages":"E971-E980"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bb/1f/cmajo.20210294.PMC9648626.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20210294","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: The mix of care provided by family physicians, specialists and palliative care physicians can vary by the illnesses leading to death, which may result in disruptions of continuity of care at the end of life. We measured continuity of outpatient physician care in the last year of life across differing causes of death and assessed factors associated with higher continuity.
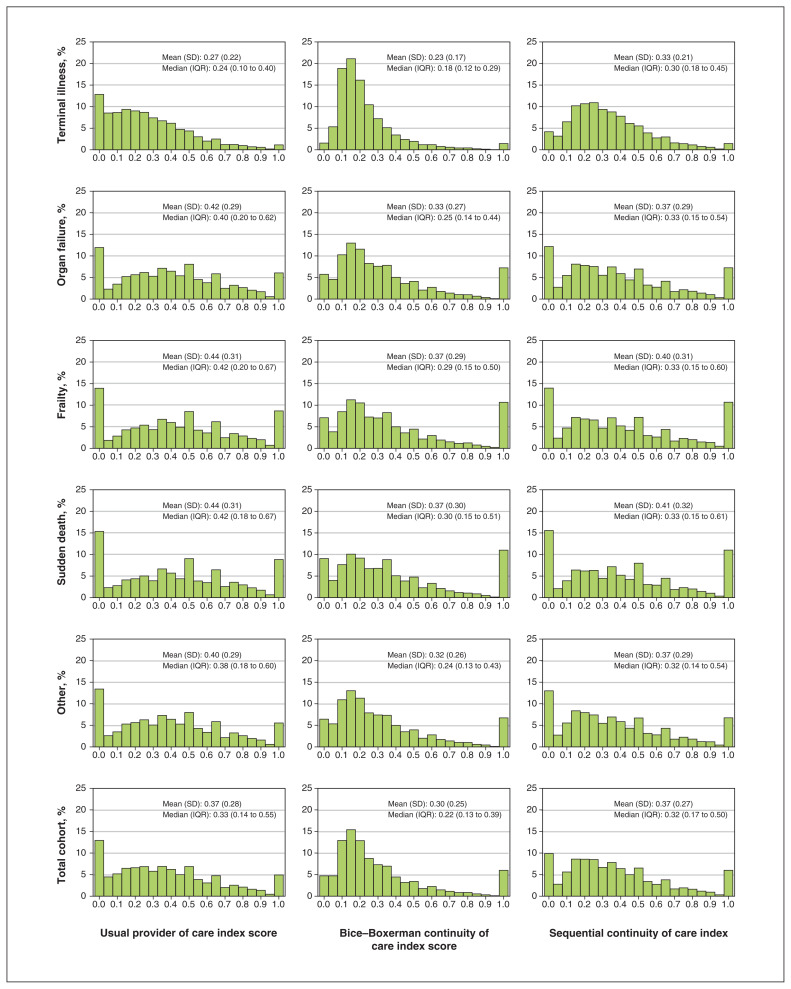
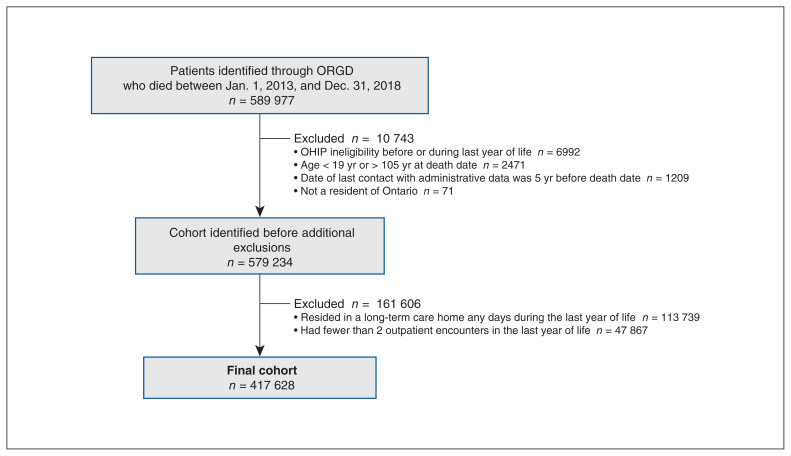
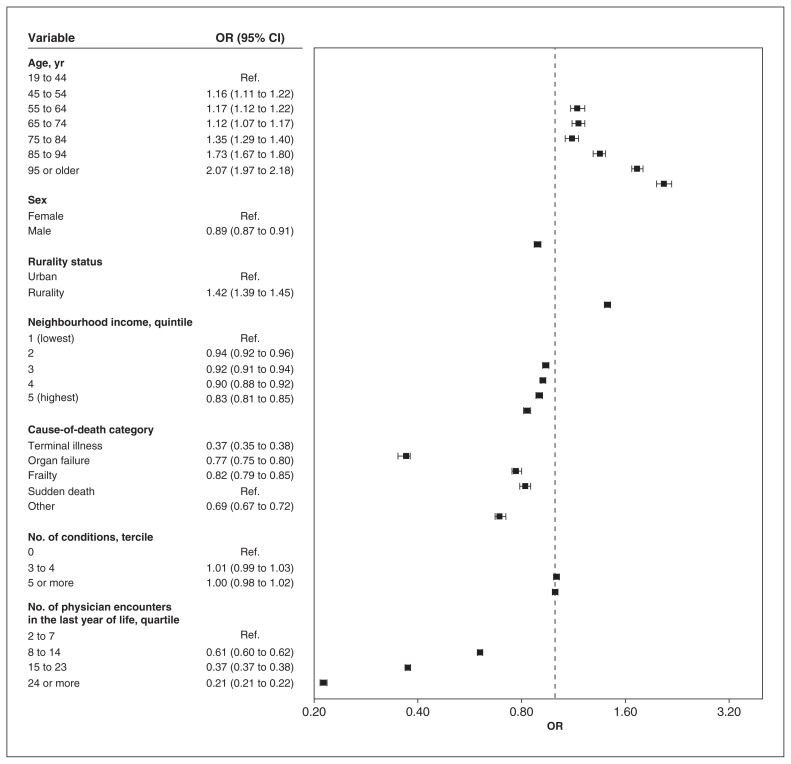
Methods: We conducted a retrospective descriptive study of adults who died in Ontario between 2013 and 2018, using linked provincial health administrative data. We calculated 3 measures of continuity (usual provider, Bice-Boxerman and sequential continuity), which range from 0 to 1, from outpatient physician visits over the last year of life for terminal illness, organ failure, frailty, sudden death and other causes of death. We used multivariable logistic regression models to evaluate associations between characteristics and a continuity score of 0.5 or greater.
Results: Among the 417 628 decedents, we found that mean usual provider, Bice-Boxerman and sequential continuity indices were 0.37, 0.30 and 0.37, respectively, with continuity being the lowest for those with terminal illness (0.27, 0.23 and 0.33, respectively). Higher number of comorbidities, higher neighbourhood income quintile and all non-sudden death categories were associated with lower continuity.
Interpretation: We found that continuity of physician care in the last year of life was low, especially in those with cancer. Further research is needed to validate measures of continuity against end-of-life health care outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


