Hyemoon Chung, Sung Wan Kim, Hyung Oh Kim, Jung Myung Lee, Jong Shin Woo, Jin Bae Kim, Soo Joong Kim, Weon Kim, Kwon Sam Kim, Woo-Shik Kim
{"title":"Reduced Coronary Flow Reserve Is Associated with Impaired Ventricular-vascular Interaction in Patients with Obstructive Sleep Apnea.","authors":"Hyemoon Chung, Sung Wan Kim, Hyung Oh Kim, Jung Myung Lee, Jong Shin Woo, Jin Bae Kim, Soo Joong Kim, Weon Kim, Kwon Sam Kim, Woo-Shik Kim","doi":"10.36628/ijhf.2020.0005","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Obstructive sleep apnea (OSA) is associated with cardiac and arterial damage and adverse cardiovascular outcomes. We aimed to determine whether coronary flow reserve (CFR), which represents microvascular dysfunction, might be associated with the ventricular-vascular coupling index (VVI), which represents the afterload-adjusted contractility in patients with OSA.</p><p><strong>Methods: </strong>We enrolled 281 patients (257 males; mean age, 43±11 years) with newly diagnosed OSA. Transthoracic echocardiography was performed, and adenosine-associated CFR was measured in the left anterior descending coronary artery. We evaluated the differences between the patients with normal CFR ≥2.5 and reduced CFR <2.5. VVI was calculated using the effective arterial elastance (Ea) and left ventricular (LV) end-systolic elastance (Ees) as follows: 10×Ea/Ees.</p><p><strong>Results: </strong>The normal CFR group (n=214) showed increased Ees (7.28±2.31 vs. 8.14±2.33 mmHg/mL, p=0.016) and preserved VVI (3.17±1.53 vs. 2.78±1.20, p=0.044) compared with the reduced CFR group (n=67). There were no differences in LV dimension, LV ejection fraction, left atrial-volume index, E/e', left atrial strain and LV global longitudinal strain between the 2 groups (all p>0.05). CFR was significantly correlated to Ees (r=0.139; p=0.023) and VVI (r=-0.137; p=0.025).</p><p><strong>Conclusions: </strong>Reduced CFR is associated with decreased Ees and impaired VVI in OSA patients. It suggests the necessity of more intensive observation in OSA patients with reduced CFR to improve cardiovascular outcomes.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"2 3","pages":"195-203"},"PeriodicalIF":0.0000,"publicationDate":"2020-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/96/2d/ijhf-2-195.PMC9536679.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background and objectives: Obstructive sleep apnea (OSA) is associated with cardiac and arterial damage and adverse cardiovascular outcomes. We aimed to determine whether coronary flow reserve (CFR), which represents microvascular dysfunction, might be associated with the ventricular-vascular coupling index (VVI), which represents the afterload-adjusted contractility in patients with OSA.
Methods: We enrolled 281 patients (257 males; mean age, 43±11 years) with newly diagnosed OSA. Transthoracic echocardiography was performed, and adenosine-associated CFR was measured in the left anterior descending coronary artery. We evaluated the differences between the patients with normal CFR ≥2.5 and reduced CFR <2.5. VVI was calculated using the effective arterial elastance (Ea) and left ventricular (LV) end-systolic elastance (Ees) as follows: 10×Ea/Ees.
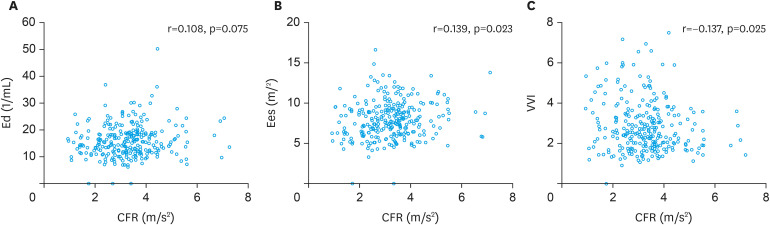
Results: The normal CFR group (n=214) showed increased Ees (7.28±2.31 vs. 8.14±2.33 mmHg/mL, p=0.016) and preserved VVI (3.17±1.53 vs. 2.78±1.20, p=0.044) compared with the reduced CFR group (n=67). There were no differences in LV dimension, LV ejection fraction, left atrial-volume index, E/e', left atrial strain and LV global longitudinal strain between the 2 groups (all p>0.05). CFR was significantly correlated to Ees (r=0.139; p=0.023) and VVI (r=-0.137; p=0.025).
Conclusions: Reduced CFR is associated with decreased Ees and impaired VVI in OSA patients. It suggests the necessity of more intensive observation in OSA patients with reduced CFR to improve cardiovascular outcomes.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


