Joelizy Oliveira, Thaís Costa E Silva, Ana C Cabral, Marta Lavrador, Filipe F Almeida, António Macedo, Carlos Saraiva, Fernando Fernandez-Llimos, M Margarida Caramona, Isabel V Figueiredo, M Margarida Castel-Branco
{"title":"Pharmacist-led medication reconciliation on admission to an acute psychiatric hospital unit.","authors":"Joelizy Oliveira, Thaís Costa E Silva, Ana C Cabral, Marta Lavrador, Filipe F Almeida, António Macedo, Carlos Saraiva, Fernando Fernandez-Llimos, M Margarida Caramona, Isabel V Figueiredo, M Margarida Castel-Branco","doi":"10.18549/PharmPract.2022.2.2650","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Therapy management in patients suffering from mental health disorders is complex and the risks derived from changes or interruptions of treatment should not be ignored. Medication reconciliation in psychiatry may reduce medication errors and promote patient safety during transitions of care.</p><p><strong>Objective: </strong>To identify the influence of complementary information sources in the construction of the best possible medication history, and to ascertain the potential clinical impact of discrepancies identified in a medication reconciliation service.</p><p><strong>Methods: </strong>An observational study was conducted in an acute mental hospital unit, with a further validation in an internal medicine unit. Adult patients taking at least one medicine admitted in the unit were included. Patients/caregivers were interviewed upon admission and the information gathered was compared with hospital medical and shared electronic medical records. Once the best possible medication history was gathered, therapeutic information was reconciled against the prescription on admission to identify discrepancies. Potential clinical impact of medication errors was classified using the International Safety Classification.</p><p><strong>Results: </strong>During the study period, 148 patients were admitted, 50.7% females, mean age 54.6 years (SD=16.3). Collaboration of a caregiver was a needed in 74% of the interviews. In total, 1,147 drugs were considered to obtain patients' best possible medication history. After reconciliation, 560 clinically sound intentional discrepancies were identified and 359 discrepancies required further clarification from prescribers: 84.12% \"drug omission\", 5.57% \"drug substitution\", 6.96% \"dose change\", and 3.34% \"dosage frequency change\". Potential clinical impact of these medication discrepancies was classified as: 95 mild, 100 moderate, and 29 severe medication errors.</p><p><strong>Conclusion: </strong>About 1 in three intentional discrepancies observed in a pharmacists-led medication reconciliation service required further clarification from prescribers, being 80% of them unintentional discrepancies. Results highlight the importance of the caregiver as source of information for the psychiatric patient, the relevance of analyzing shared electronic health records until 6 months before, and the need to use hospital medical records efficiently. Additionally, 29 discrepancies were classified as errors with potentially severe clinical impact. A medication reconciliation service is concluded to be feasible and necessary in a mental health unit.</p>","PeriodicalId":51762,"journal":{"name":"Pharmacy Practice-Granada","volume":"20 2","pages":"2650"},"PeriodicalIF":1.0000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0e/9d/pharmpract-20-2650.PMC9296076.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacy Practice-Granada","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18549/PharmPract.2022.2.2650","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/3/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Therapy management in patients suffering from mental health disorders is complex and the risks derived from changes or interruptions of treatment should not be ignored. Medication reconciliation in psychiatry may reduce medication errors and promote patient safety during transitions of care.
Objective: To identify the influence of complementary information sources in the construction of the best possible medication history, and to ascertain the potential clinical impact of discrepancies identified in a medication reconciliation service.
Methods: An observational study was conducted in an acute mental hospital unit, with a further validation in an internal medicine unit. Adult patients taking at least one medicine admitted in the unit were included. Patients/caregivers were interviewed upon admission and the information gathered was compared with hospital medical and shared electronic medical records. Once the best possible medication history was gathered, therapeutic information was reconciled against the prescription on admission to identify discrepancies. Potential clinical impact of medication errors was classified using the International Safety Classification.
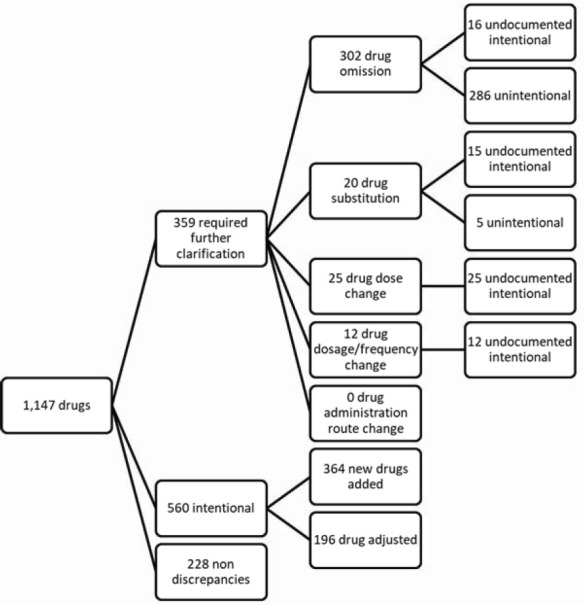
Results: During the study period, 148 patients were admitted, 50.7% females, mean age 54.6 years (SD=16.3). Collaboration of a caregiver was a needed in 74% of the interviews. In total, 1,147 drugs were considered to obtain patients' best possible medication history. After reconciliation, 560 clinically sound intentional discrepancies were identified and 359 discrepancies required further clarification from prescribers: 84.12% "drug omission", 5.57% "drug substitution", 6.96% "dose change", and 3.34% "dosage frequency change". Potential clinical impact of these medication discrepancies was classified as: 95 mild, 100 moderate, and 29 severe medication errors.
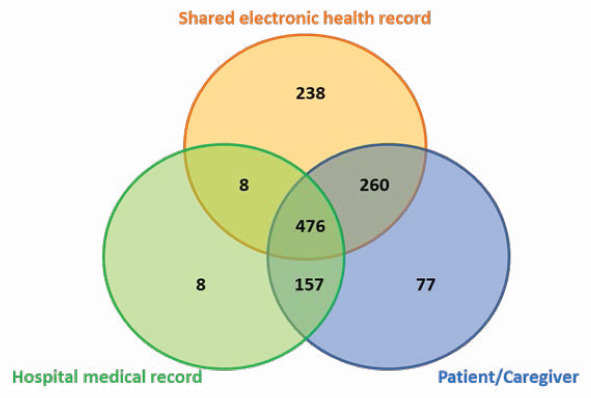
Conclusion: About 1 in three intentional discrepancies observed in a pharmacists-led medication reconciliation service required further clarification from prescribers, being 80% of them unintentional discrepancies. Results highlight the importance of the caregiver as source of information for the psychiatric patient, the relevance of analyzing shared electronic health records until 6 months before, and the need to use hospital medical records efficiently. Additionally, 29 discrepancies were classified as errors with potentially severe clinical impact. A medication reconciliation service is concluded to be feasible and necessary in a mental health unit.
期刊介绍:
Pharmacy Practice is a free full-text peer-reviewed journal with a scope on pharmacy practice. Pharmacy Practice is published quarterly. Pharmacy Practice does not charge and will never charge any publication fee or article processing charge (APC) to the authors. The current and future absence of any article processing charges (APCs) is signed in the MoU with the Center for Pharmacy Practice Innovation (CPPI) at Virginia Commonwealth University (VCU) School of Pharmacy. Pharmacy Practice is the consequence of the efforts of a number of colleagues from different Universities who belief in collaborative publishing: no one pays, no one receives. Although focusing on the practice of pharmacy, Pharmacy Practice covers a wide range of pharmacy activities, among them and not being comprehensive, clinical pharmacy, pharmaceutical care, social pharmacy, pharmacy education, process and outcome research, health promotion and education, health informatics, pharmacoepidemiology, etc.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


