Results of a multi-site pragmatic hybrid type 3 cluster randomized trial comparing level of facilitation while implementing an intervention in community-dwelling disabled and older adults in a Medicaid waiver.
Sandra L Spoelstra, Monica Schueller, Viktoria Basso, Alla Sikorskii
{"title":"Results of a multi-site pragmatic hybrid type 3 cluster randomized trial comparing level of facilitation while implementing an intervention in community-dwelling disabled and older adults in a Medicaid waiver.","authors":"Sandra L Spoelstra, Monica Schueller, Viktoria Basso, Alla Sikorskii","doi":"10.1186/s13012-022-01232-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evidence-based interventions that optimize physical function for disabled and older adults living in the community who have difficulty with daily living tasks are available. However, uptake has been limited, particularly in resource-constrained (Medicaid) settings. Facilitation may be an effective implementation strategy. This study's aim was to compare internal facilitation (IF) versus IF and external facilitation (EF) on adoption and sustainability of an intervention in a Medicaid home and community-based waiver.</p><p><strong>Methods: </strong>In a hybrid type 3 trial, waiver sites (N = 18) were randomly assigned to implement the intervention using a bundle of strategies with either IF or IF and EF. Adoption and sustainability were assessed via Stages of Implementation Completion (SIC) for each site. Clinician attitudes toward evidence-based practice and self-efficacy were evaluated among 539 registered nurses, social workers, and occupational therapists. Medicaid beneficiary outcomes of activities of daily living, depression, pain, falls, emergency department visits, and hospitalizations were evaluated in a sample of N = 7030 as reflected by electronic health records data of the Medicaid waiver program. Linear mixed-effects models were used to compare outcomes between trial arms while accounting for cluster-randomized design.</p><p><strong>Results: </strong>The mean SIC scores were 72.22 (standard deviation [SD] = 16.98) in the IF arm (9 sites) and 61.33 (SD = 19.29) in the IF + EF arm (9 sites). The difference was not statistically significant but corresponded to the medium clinically important effect size Cohen's d = 0.60. Clinician implementation outcomes of attitudes and self-efficacy did not differ by trial arm. Beneficiary depression was reduced significantly in the IF + EF arm compared to the IF arm (p = .04, 95% confidence interval for the difference [0.01, 0.24]). No differences between trial arms were found for other beneficiary outcomes.</p><p><strong>Conclusions: </strong>Level of facilitation did not enhance capacity for adoption and sustainability of an evidence-based intervention in a Medicaid setting that cares for disabled and older adults. Improved beneficiary depression favored use of IF and EF compared to IF alone, and no differences were found for other outcomes. These findings also suggest level of facilitation may not have impacted beneficiary outcomes.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov , NCT03634033 ; date registered August 16, 2018.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"57"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9419328/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13012-022-01232-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Evidence-based interventions that optimize physical function for disabled and older adults living in the community who have difficulty with daily living tasks are available. However, uptake has been limited, particularly in resource-constrained (Medicaid) settings. Facilitation may be an effective implementation strategy. This study's aim was to compare internal facilitation (IF) versus IF and external facilitation (EF) on adoption and sustainability of an intervention in a Medicaid home and community-based waiver.
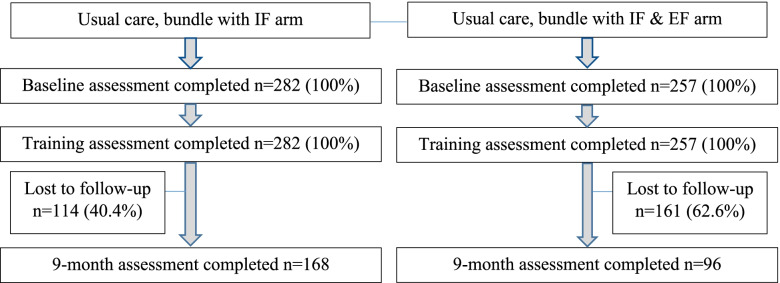
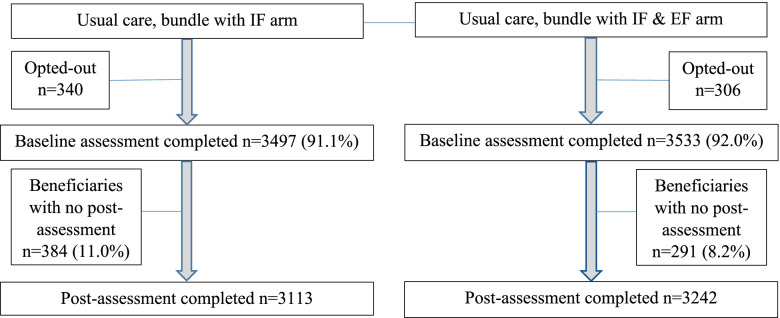
Methods: In a hybrid type 3 trial, waiver sites (N = 18) were randomly assigned to implement the intervention using a bundle of strategies with either IF or IF and EF. Adoption and sustainability were assessed via Stages of Implementation Completion (SIC) for each site. Clinician attitudes toward evidence-based practice and self-efficacy were evaluated among 539 registered nurses, social workers, and occupational therapists. Medicaid beneficiary outcomes of activities of daily living, depression, pain, falls, emergency department visits, and hospitalizations were evaluated in a sample of N = 7030 as reflected by electronic health records data of the Medicaid waiver program. Linear mixed-effects models were used to compare outcomes between trial arms while accounting for cluster-randomized design.
Results: The mean SIC scores were 72.22 (standard deviation [SD] = 16.98) in the IF arm (9 sites) and 61.33 (SD = 19.29) in the IF + EF arm (9 sites). The difference was not statistically significant but corresponded to the medium clinically important effect size Cohen's d = 0.60. Clinician implementation outcomes of attitudes and self-efficacy did not differ by trial arm. Beneficiary depression was reduced significantly in the IF + EF arm compared to the IF arm (p = .04, 95% confidence interval for the difference [0.01, 0.24]). No differences between trial arms were found for other beneficiary outcomes.
Conclusions: Level of facilitation did not enhance capacity for adoption and sustainability of an evidence-based intervention in a Medicaid setting that cares for disabled and older adults. Improved beneficiary depression favored use of IF and EF compared to IF alone, and no differences were found for other outcomes. These findings also suggest level of facilitation may not have impacted beneficiary outcomes.
Trial registration: ClinicalTrials.gov , NCT03634033 ; date registered August 16, 2018.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


