Ming-Hao Luo, Jing-Chao Luo, Yi-Jie Zhang, Xin Xu, Ying Su, Jia-Kun Li, Chun-Sheng Wang, Hao Lai, Yong-Xin Sun, Jun Li, Guo-Wei Tu, Zhe Luo
{"title":"Early postoperative organ dysfunction is highly associated with the mortality risk of patients with type A aortic dissection.","authors":"Ming-Hao Luo, Jing-Chao Luo, Yi-Jie Zhang, Xin Xu, Ying Su, Jia-Kun Li, Chun-Sheng Wang, Hao Lai, Yong-Xin Sun, Jun Li, Guo-Wei Tu, Zhe Luo","doi":"10.1093/icvts/ivac266","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study assessed the impact of early postoperative organ dysfunction (EPOD) on in-hospital mortality of patients with type A aortic dissection (TAAD) after surgery.</p><p><strong>Methods: </strong>Patients with TAAD who underwent surgical repair requiring deep hypothermic circulatory arrest from January 2020 to December 2021 were included. The Sequential Organ Failure Assessment (SOFA) score was calculated for 3 days postoperatively to stratify the severity of organ dysfunction. Patients with the SOFA of 0-4, 5-8 or >8 were defined as mild, moderate or severe EPOD. The primary outcome was in-hospital mortality, and a composite secondary outcome was defined as in-hospital death or any major complications. Kaplan-Meier curves were used to compare survival probability. The area under the receiver operating characteristic curve and calibration plots were used to evaluate the predictive power and overall performance of SOFA.</p><p><strong>Results: </strong>Of the 368 patients, 5 patients (3%) with moderate EPOD and 33 patients (23%) with severe EPOD died. No patient died with mild EPOD. The areas under the receiver operating characteristic curve of SOFA for predicting mortality and the composite outcome were 0.85 (0.81-0.88) and 0.81 (0.77-0.85) on postoperative day 1. Each point of postoperative day 1 SOFA score corresponded to an odds ratio of 1.65 (1.42-1.92) for mortality. Of the 6 components of the SOFA system, only coagulation (2.34 [1.32-4.13]), cardiovascular (1.47 [1.04-2.08]), central nervous system (1.96 [1.36-2.82]) and renal (1.67 [1.04-2.70]) functions were associated with the higher risk of mortality.</p><p><strong>Conclusions: </strong>EPOD stratified by the SOFA score was associated with a higher risk of death and predicted the clinical outcomes of patients with TAAD with good accuracy.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9642332/pdf/","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac266","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 4
Abstract
Objectives: This study assessed the impact of early postoperative organ dysfunction (EPOD) on in-hospital mortality of patients with type A aortic dissection (TAAD) after surgery.
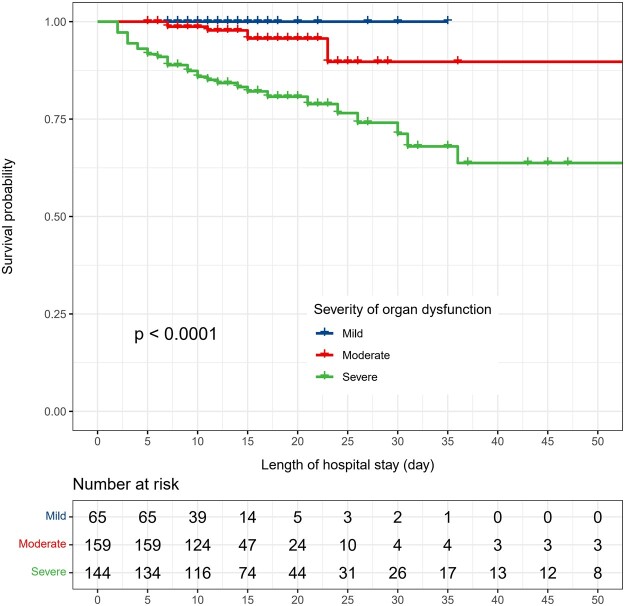
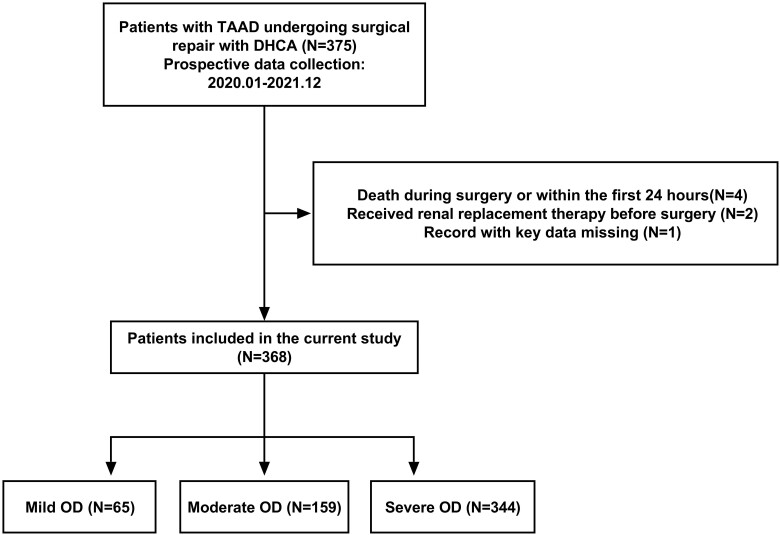
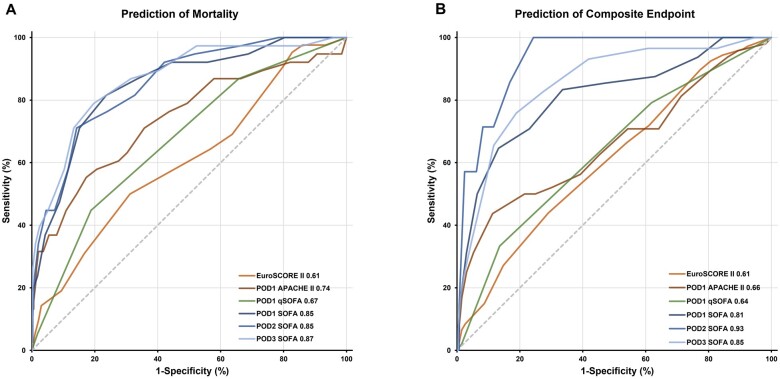
Methods: Patients with TAAD who underwent surgical repair requiring deep hypothermic circulatory arrest from January 2020 to December 2021 were included. The Sequential Organ Failure Assessment (SOFA) score was calculated for 3 days postoperatively to stratify the severity of organ dysfunction. Patients with the SOFA of 0-4, 5-8 or >8 were defined as mild, moderate or severe EPOD. The primary outcome was in-hospital mortality, and a composite secondary outcome was defined as in-hospital death or any major complications. Kaplan-Meier curves were used to compare survival probability. The area under the receiver operating characteristic curve and calibration plots were used to evaluate the predictive power and overall performance of SOFA.
Results: Of the 368 patients, 5 patients (3%) with moderate EPOD and 33 patients (23%) with severe EPOD died. No patient died with mild EPOD. The areas under the receiver operating characteristic curve of SOFA for predicting mortality and the composite outcome were 0.85 (0.81-0.88) and 0.81 (0.77-0.85) on postoperative day 1. Each point of postoperative day 1 SOFA score corresponded to an odds ratio of 1.65 (1.42-1.92) for mortality. Of the 6 components of the SOFA system, only coagulation (2.34 [1.32-4.13]), cardiovascular (1.47 [1.04-2.08]), central nervous system (1.96 [1.36-2.82]) and renal (1.67 [1.04-2.70]) functions were associated with the higher risk of mortality.
Conclusions: EPOD stratified by the SOFA score was associated with a higher risk of death and predicted the clinical outcomes of patients with TAAD with good accuracy.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


