Hoe Jeong Chung, Doo Sup Kim, Jin Woo Lee, Seok In Hong
{"title":"Analyzing the Risk Factors of Mortality after Osteoporotic Hip Fractures Using the National Health Insurance Service Sample Cohort 2.0 Database.","authors":"Hoe Jeong Chung, Doo Sup Kim, Jin Woo Lee, Seok In Hong","doi":"10.5371/hp.2022.34.3.150","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The purpose of this study is to determine risk factors that affect mortality following osteoporotic hip fracture in patients 50 years or older using the National Health Insurance Service (NHIS) sample cohort 2.0 database.</p><p><strong>Materials and methods: </strong>Data from 2,533 patients who satisfied the inclusion criteria for the NHIS sample cohort 2.0 database were used in this study. Data from patients who suffered osteoporotic hip fractures between 2002-2015 were used. An analysis of correlations between the incidence of osteoporotic hip fractures and various factors (sex, age, underlying diseases, etc.) was performed. Analysis of the associations between the mortality of osteoporotic hip fracture and the various factors with hazard ratio (HR) was performed using Cox regression models.</p><p><strong>Results: </strong>Patient observation continued for an average of 38.12±32.09 months. During the observation period, a higher incidence of hip fracture was observed in women; however, higher mortality following the fracture was observed in men (HR=0.728; 95% confidence interval [CI], 0.635-0.836). The incidence and mortality of fractures increased when there were increasing age, more than three underlying diseases (HR=1.945; 95% CI, 1.284-2.945), cerebrovascular diseases (HR=1.429; 95% CI, 1.232-1.657), and renal diseases (HR=1.248; 95% CI, 1.040-1.497). Also, higher mortality was observed in patients who were underweight (HR=1.342; 95% CI, 1.079-1.669), current smokers (HR=1.338; 95% CI, 1.104-1.621), and inactivity (HR=1.379; 95% CI, 1.189-1.601).</p><p><strong>Conclusion: </strong>Male gender, the presence of cerebrovascular or kidney disease, a more than three underlying diseases, underweight, a current smoker, and inactivity were risk factors that increased mortality.</p>","PeriodicalId":73239,"journal":{"name":"Hip & pelvis","volume":"34 3","pages":"150-160"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/50/65/hp-34-150.PMC9577307.pdf","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hip & pelvis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5371/hp.2022.34.3.150","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
Abstract
Purpose: The purpose of this study is to determine risk factors that affect mortality following osteoporotic hip fracture in patients 50 years or older using the National Health Insurance Service (NHIS) sample cohort 2.0 database.
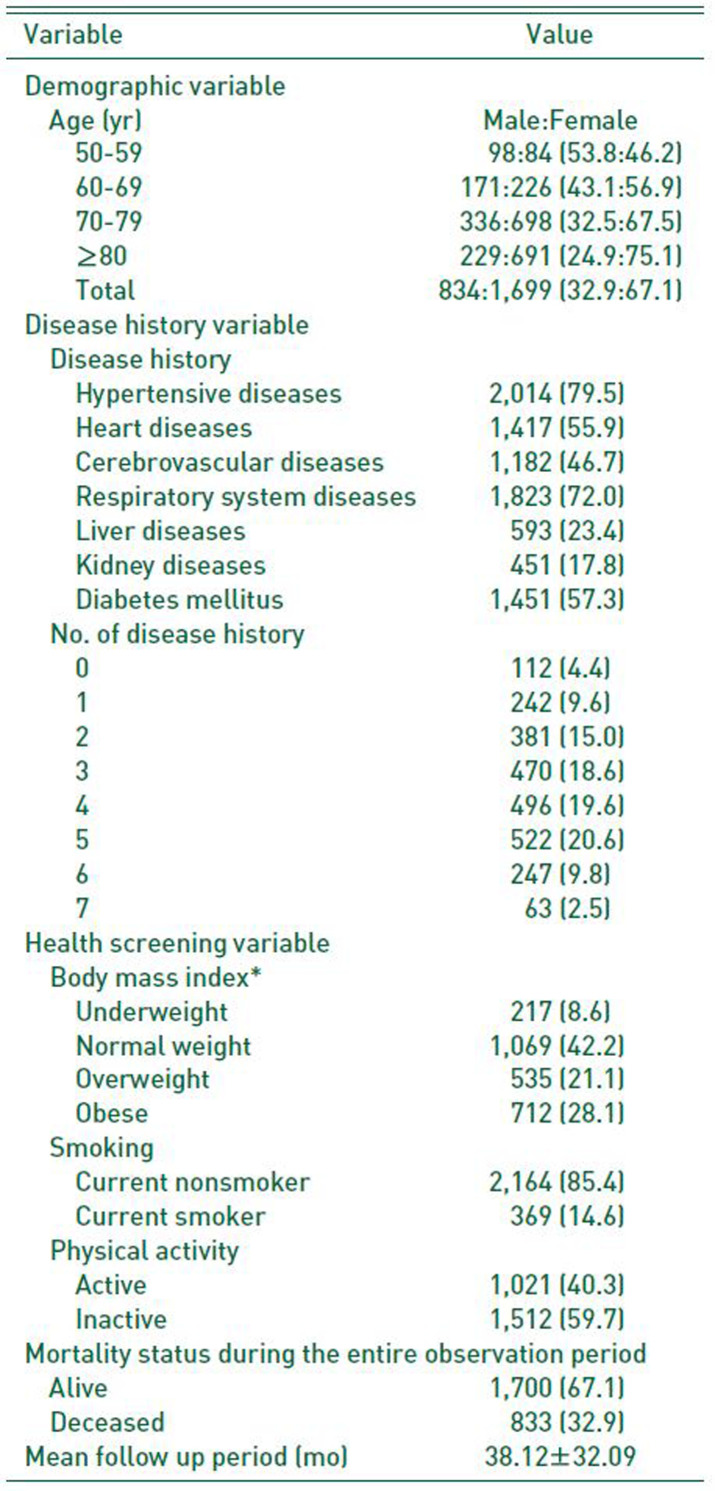
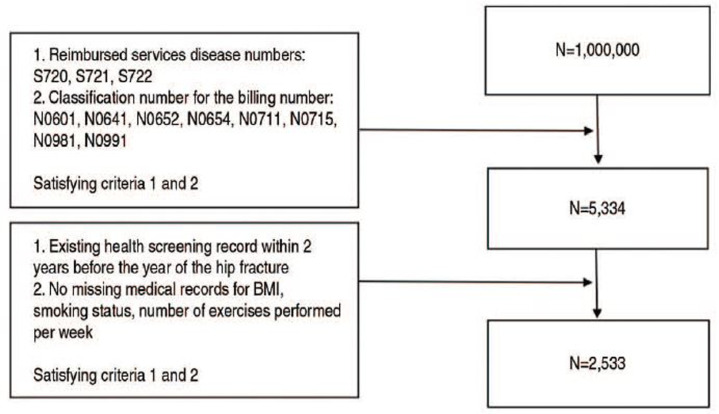
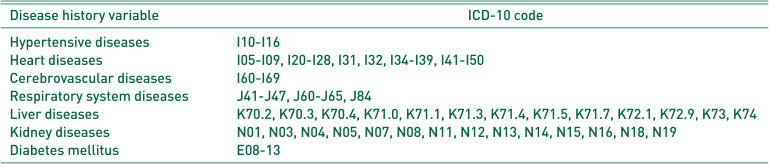
Materials and methods: Data from 2,533 patients who satisfied the inclusion criteria for the NHIS sample cohort 2.0 database were used in this study. Data from patients who suffered osteoporotic hip fractures between 2002-2015 were used. An analysis of correlations between the incidence of osteoporotic hip fractures and various factors (sex, age, underlying diseases, etc.) was performed. Analysis of the associations between the mortality of osteoporotic hip fracture and the various factors with hazard ratio (HR) was performed using Cox regression models.
Results: Patient observation continued for an average of 38.12±32.09 months. During the observation period, a higher incidence of hip fracture was observed in women; however, higher mortality following the fracture was observed in men (HR=0.728; 95% confidence interval [CI], 0.635-0.836). The incidence and mortality of fractures increased when there were increasing age, more than three underlying diseases (HR=1.945; 95% CI, 1.284-2.945), cerebrovascular diseases (HR=1.429; 95% CI, 1.232-1.657), and renal diseases (HR=1.248; 95% CI, 1.040-1.497). Also, higher mortality was observed in patients who were underweight (HR=1.342; 95% CI, 1.079-1.669), current smokers (HR=1.338; 95% CI, 1.104-1.621), and inactivity (HR=1.379; 95% CI, 1.189-1.601).
Conclusion: Male gender, the presence of cerebrovascular or kidney disease, a more than three underlying diseases, underweight, a current smoker, and inactivity were risk factors that increased mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


