Yoji Hoshina, Jonathan Galli, Ka-Ho Wong, Tibor Kovacsovics, Mary Steinbach, Karen L Salzman, Joseph Scott McNally, Eric Lancaster, M Mateo Paz Soldán, Stacey L Clardy
{"title":"GABA-A Receptor Encephalitis After Autologous Hematopoietic Stem Cell Transplant forMultiple Myeloma: Three Cases and Literature Review.","authors":"Yoji Hoshina, Jonathan Galli, Ka-Ho Wong, Tibor Kovacsovics, Mary Steinbach, Karen L Salzman, Joseph Scott McNally, Eric Lancaster, M Mateo Paz Soldán, Stacey L Clardy","doi":"10.1212/NXI.0000000000200024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>The relationship between autologous hematopoietic stem cell transplant (aHSCT) for multiple myeloma (MM) and anti-GABA<sub>A</sub> receptor (GABA<sub>A</sub>R) encephalitis is unknown. We aimed to describe the clinical features, diagnostic process, and outcome of 3 cases of anti-GABA<sub>A</sub>R encephalitis in patients with a history of prior aHSCT for MM.</p><p><strong>Methods: </strong>A case series of 3 patients. Anti-GABA<sub>A</sub>R antibody was tested at the University of Pennsylvania Laboratory.</p><p><strong>Results: </strong>The patients were all male, aged 52 (case 1), 61 (case 2), and 62 (case 3) years at encephalitis symptom onset. The duration between completion of aHSCT and the onset of encephalitis was 43, 18, and 9 months, respectively. All 3 patients presented with new seizures and altered cognitive function. Other symptoms included headache and visual obscurations in cases 1 and 2 and intractable vertigo and mania in case 3. Brain MRI demonstrated nonenhancing multifocal T2-weighted/fluid-attenuated inversion recovery cortical and subcortical hyperintensities in all 3 patients. Cases 2 and 3 underwent brain biopsy before initiating immunomodulatory therapy, which demonstrated nonspecific encephalitis with astrogliosis in the white matter; these 2 patients were started on immunotherapy for the treatment of anti-GABA<sub>A</sub>R encephalitis after 22 days and 3 months, respectively, from the first presentation. Case 1 was started on empiric immunotherapy within 8 days of presentation without requiring brain biopsy, given characteristic MRI imaging. CSF analysis demonstrated the presence of anti-GABA<sub>A</sub>R antibodies in all 3 cases. Cases 1 and 3 also tested positive for anti-GABA<sub>A</sub>R antibodies in the serum (serum test was not performed in case 2). Cases 1 and 2 recovered to work full-time within 1 year. Case 3 reported occasional myoclonic-like movement.</p><p><strong>Discussion: </strong>We highlight the importance of considering anti-GABA<sub>A</sub>R encephalitis in patients with seizures, multifocal nonenhancing brain lesions, and a history of aHSCT for MM. Awareness in recovered post-aHSCT patients with MM may be crucial because prompt recognition can avoid brain biopsy and delays in treatment. The rapid initiation of immunotherapy while awaiting autoantibody results will likely improve functional outcomes.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d7/2d/NXI-2022-200030.PMC9417160.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: The relationship between autologous hematopoietic stem cell transplant (aHSCT) for multiple myeloma (MM) and anti-GABAA receptor (GABAAR) encephalitis is unknown. We aimed to describe the clinical features, diagnostic process, and outcome of 3 cases of anti-GABAAR encephalitis in patients with a history of prior aHSCT for MM.
Methods: A case series of 3 patients. Anti-GABAAR antibody was tested at the University of Pennsylvania Laboratory.
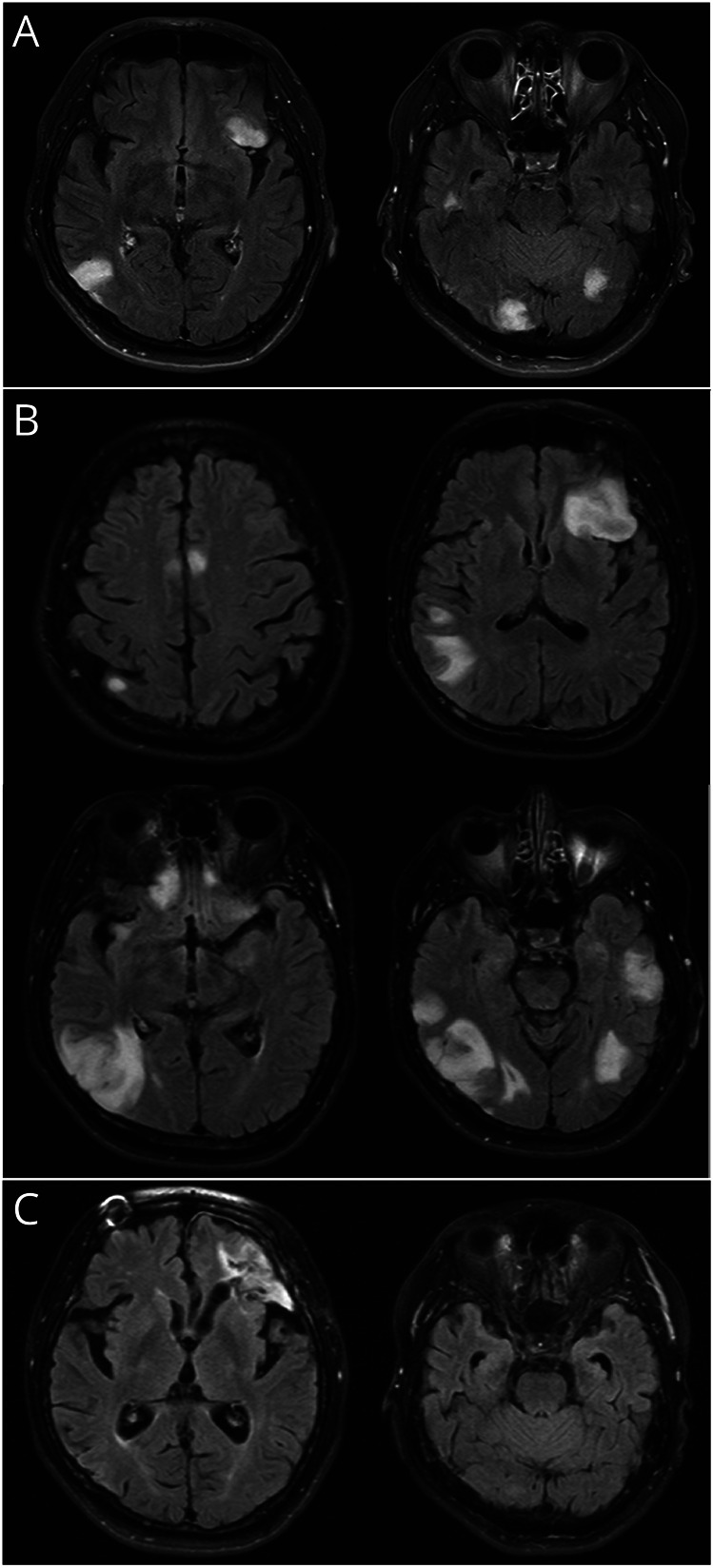
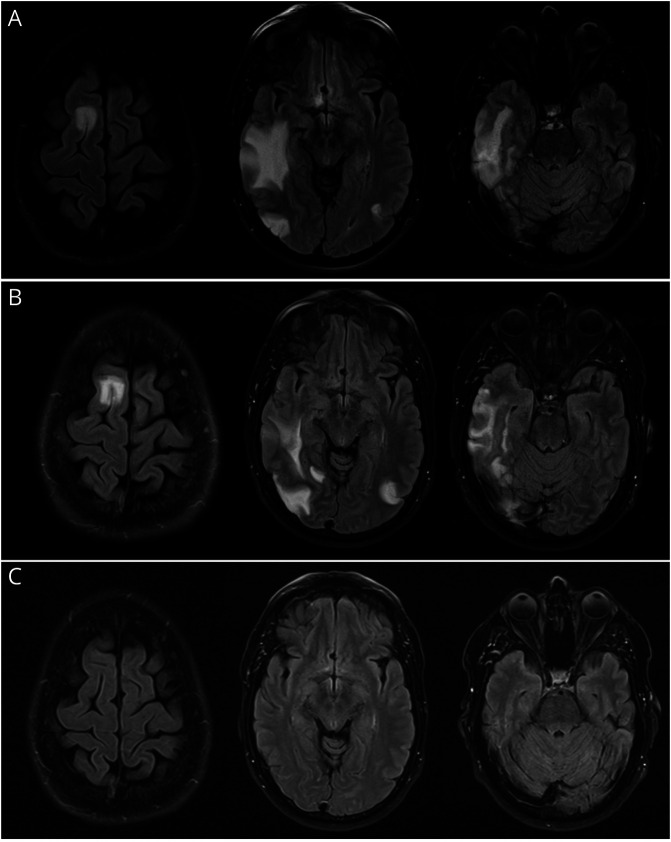
Results: The patients were all male, aged 52 (case 1), 61 (case 2), and 62 (case 3) years at encephalitis symptom onset. The duration between completion of aHSCT and the onset of encephalitis was 43, 18, and 9 months, respectively. All 3 patients presented with new seizures and altered cognitive function. Other symptoms included headache and visual obscurations in cases 1 and 2 and intractable vertigo and mania in case 3. Brain MRI demonstrated nonenhancing multifocal T2-weighted/fluid-attenuated inversion recovery cortical and subcortical hyperintensities in all 3 patients. Cases 2 and 3 underwent brain biopsy before initiating immunomodulatory therapy, which demonstrated nonspecific encephalitis with astrogliosis in the white matter; these 2 patients were started on immunotherapy for the treatment of anti-GABAAR encephalitis after 22 days and 3 months, respectively, from the first presentation. Case 1 was started on empiric immunotherapy within 8 days of presentation without requiring brain biopsy, given characteristic MRI imaging. CSF analysis demonstrated the presence of anti-GABAAR antibodies in all 3 cases. Cases 1 and 3 also tested positive for anti-GABAAR antibodies in the serum (serum test was not performed in case 2). Cases 1 and 2 recovered to work full-time within 1 year. Case 3 reported occasional myoclonic-like movement.
Discussion: We highlight the importance of considering anti-GABAAR encephalitis in patients with seizures, multifocal nonenhancing brain lesions, and a history of aHSCT for MM. Awareness in recovered post-aHSCT patients with MM may be crucial because prompt recognition can avoid brain biopsy and delays in treatment. The rapid initiation of immunotherapy while awaiting autoantibody results will likely improve functional outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


