{"title":"Spinal Epidural Hematoma Due to Venous Congestion Caused by Nutcracker Syndrome.","authors":"Hiroyuki Mishima, Junichi Ayabe, Mutsumi Takadera, Yusuke Tsuchiya, Taisuke Kawasaki, Masayuki Okano, Masanori Isoda, Yoshihide Tanaka","doi":"10.2176/jns-nmc.2022-0066","DOIUrl":null,"url":null,"abstract":"<p><p>The causes of spinal epidural hematoma (SEH) have been attributed to coagulopathy, trauma, vascular anomalies, and so forth. The incidence of vascular anomalies shown by digital subtraction angiography has been reported to be 15%, and most cases have been reported to be spinal epidural arteriovenous fistulae. SEH has rarely been caused by venous congestion. We report a case of SEH in a 78-year-old male who presented to our emergency department with sudden-onset back pain, followed by complete paraplegia with bladder and rectal disturbance. Magnetic resonance imaging revealed a dorsally placed extradural hematoma extending from T10 to L1. An urgent laminectomy from T11 to L2 was performed. Computed tomography angiography (CTA) performed 1 week after the operation showed compression of the left renal vein between the aorta and superior mesenteric artery with dilation of the surrounding veins, including the spinal epidural venous plexus, at the same level as the hematoma. This was diagnosed as Nutcracker syndrome (NCS), which was consistent as a cause of SEH. The patient's symptoms gradually improved, and after 6 months, he regained normal strength in his lower extremities, but bladder and rectal disturbance remained and required intermittent self-catheterization. We chose conservative treatment for NCS, and SEH did not recur until the patient died of a cause unrelated to SEH or NCS. SEH could occur secondary to venous congestion including NCS. We emphasize the importance of investigating venous return to evaluate the etiology of SEH, which can be clearly visualized using CTA.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":" ","pages":"209-212"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8b/2a/2188-4226-9-0209.PMC9339261.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
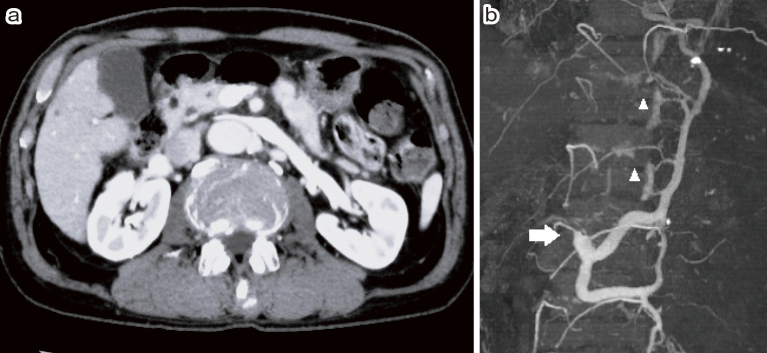
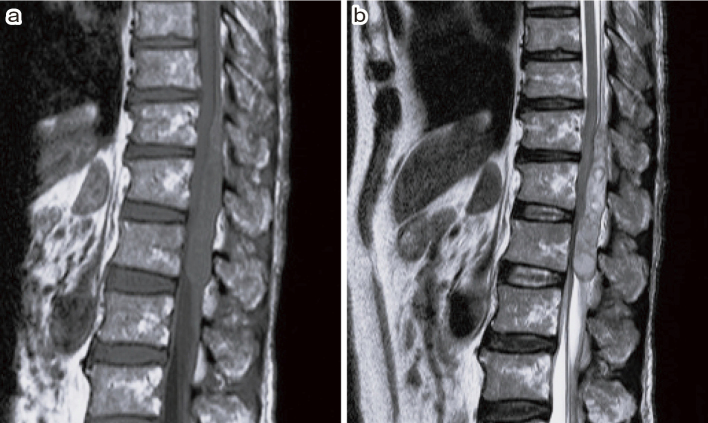
The causes of spinal epidural hematoma (SEH) have been attributed to coagulopathy, trauma, vascular anomalies, and so forth. The incidence of vascular anomalies shown by digital subtraction angiography has been reported to be 15%, and most cases have been reported to be spinal epidural arteriovenous fistulae. SEH has rarely been caused by venous congestion. We report a case of SEH in a 78-year-old male who presented to our emergency department with sudden-onset back pain, followed by complete paraplegia with bladder and rectal disturbance. Magnetic resonance imaging revealed a dorsally placed extradural hematoma extending from T10 to L1. An urgent laminectomy from T11 to L2 was performed. Computed tomography angiography (CTA) performed 1 week after the operation showed compression of the left renal vein between the aorta and superior mesenteric artery with dilation of the surrounding veins, including the spinal epidural venous plexus, at the same level as the hematoma. This was diagnosed as Nutcracker syndrome (NCS), which was consistent as a cause of SEH. The patient's symptoms gradually improved, and after 6 months, he regained normal strength in his lower extremities, but bladder and rectal disturbance remained and required intermittent self-catheterization. We chose conservative treatment for NCS, and SEH did not recur until the patient died of a cause unrelated to SEH or NCS. SEH could occur secondary to venous congestion including NCS. We emphasize the importance of investigating venous return to evaluate the etiology of SEH, which can be clearly visualized using CTA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


