{"title":"Readmission Following Perioperative Myocardial Injury: Clinical Predictors and Impact on Mortality.","authors":"Alex Anzelmi, Yasser Khalil, Martin E Matsumura","doi":"10.1155/2022/7674962","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Perioperative myocardial injury (PMI) following noncardiac surgery is associated with a high risk for mortality, and readmission within 30 days of PMI increases this risk. Identifying risk factors for readmission among survivors of PMI is critical to improving outcomes in PMI. We examined risk factors for readmission following discharge after surgery complicated by PMI and the effect of readmission on 1-year mortality.</p><p><strong>Methods: </strong>The study is a retropective cohort analysis of patients diagnosed with PMI in a single health system over a 10-year period. Univariate predictors of readmission were used to construct a multivariable logistic regression model. Mortality was assessed using Kaplan-Meyer survival analysis.</p><p><strong>Results: </strong>Of the 207,729 surgical patients, 5159 (2.5%) had PMI. By 30 days following PMI, 1254 patients (24.3%) died, 1142 (22.2%) were readmitted but alive at 30 days, and 2763 patients (53.5%) were alive and had not been readmitted. Readmitted patients were older, had higher peak troponin levels, and were more likely to have prior coronary, neoplastic, lung, and kidney disease. Multivariable logistic regression revealed increasing age and peak troponin, prior cancer diagnosis, and chronic lung and kidney disease as independent predictors of readmission. Readmitted patients had higher 1-year mortality than those not readmitted (33.9% vs. 22.2%, <i>p</i> < 0.001).</p><p><strong>Conclusions: </strong>Readmission following PMI is associated with increased mortality in the following year. Patients suffering from PMI who are at risk of readmission are older, have a greater extent of myocardial injury, and are more likely to have chronic comorbidities. Identification of patients at risk of readmission following PMI is critical to improving both outcomes and utilization of hospital resources.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":" ","pages":"7674962"},"PeriodicalIF":1.8000,"publicationDate":"2022-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9392591/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/7674962","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Perioperative myocardial injury (PMI) following noncardiac surgery is associated with a high risk for mortality, and readmission within 30 days of PMI increases this risk. Identifying risk factors for readmission among survivors of PMI is critical to improving outcomes in PMI. We examined risk factors for readmission following discharge after surgery complicated by PMI and the effect of readmission on 1-year mortality.
Methods: The study is a retropective cohort analysis of patients diagnosed with PMI in a single health system over a 10-year period. Univariate predictors of readmission were used to construct a multivariable logistic regression model. Mortality was assessed using Kaplan-Meyer survival analysis.
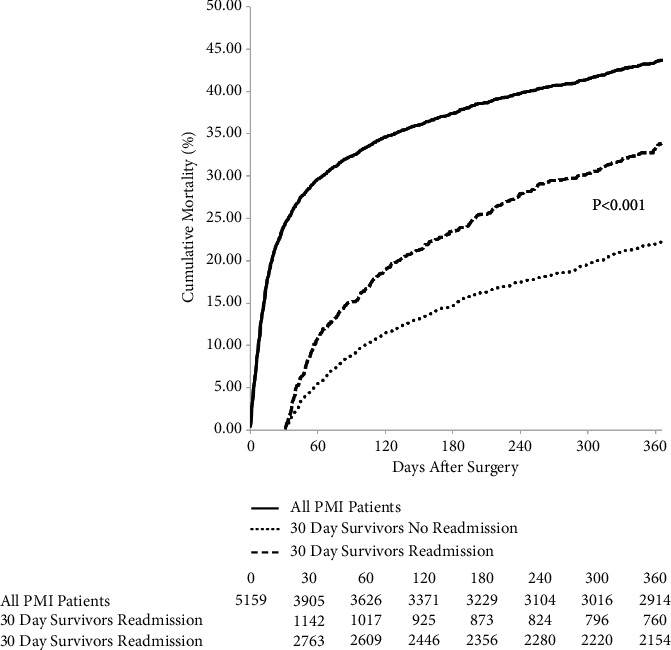
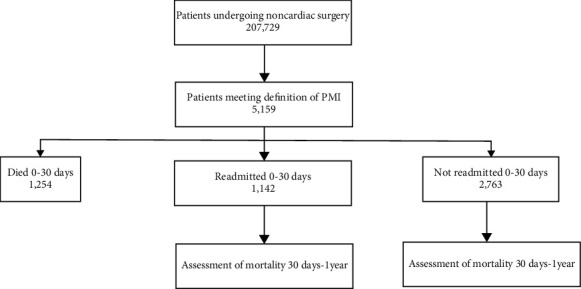
Results: Of the 207,729 surgical patients, 5159 (2.5%) had PMI. By 30 days following PMI, 1254 patients (24.3%) died, 1142 (22.2%) were readmitted but alive at 30 days, and 2763 patients (53.5%) were alive and had not been readmitted. Readmitted patients were older, had higher peak troponin levels, and were more likely to have prior coronary, neoplastic, lung, and kidney disease. Multivariable logistic regression revealed increasing age and peak troponin, prior cancer diagnosis, and chronic lung and kidney disease as independent predictors of readmission. Readmitted patients had higher 1-year mortality than those not readmitted (33.9% vs. 22.2%, p < 0.001).
Conclusions: Readmission following PMI is associated with increased mortality in the following year. Patients suffering from PMI who are at risk of readmission are older, have a greater extent of myocardial injury, and are more likely to have chronic comorbidities. Identification of patients at risk of readmission following PMI is critical to improving both outcomes and utilization of hospital resources.
背景:非心脏手术后围手术期心肌损伤(PMI)与高死亡率相关,PMI后30天内再入院增加了这一风险。确定PMI幸存者再入院的危险因素对改善PMI预后至关重要。我们检查了合并PMI的手术出院后再入院的危险因素以及再入院对1年死亡率的影响。方法:该研究是对在单一卫生系统中诊断为PMI的患者进行回顾性队列分析,为期10年。采用单变量再入院预测因子构建多变量logistic回归模型。使用Kaplan-Meyer生存分析评估死亡率。结果:在207,729例手术患者中,5159例(2.5%)有PMI。PMI后30天,1254例(24.3%)患者死亡,1142例(22.2%)患者再次入院,30天存活,2763例(53.5%)患者存活且未再次入院。再入院的患者年龄较大,肌钙蛋白峰值水平较高,既往有冠状动脉、肿瘤、肺部和肾脏疾病的可能性更大。多变量logistic回归显示,年龄增加、肌钙蛋白峰值、既往癌症诊断、慢性肺和肾脏疾病是再入院的独立预测因素。再入院患者的1年死亡率高于未再入院患者(33.9% vs. 22.2%, p < 0.001)。结论:PMI后再入院与次年死亡率增加相关。有再入院风险的PMI患者年龄较大,心肌损伤程度较大,并且更有可能患有慢性合并症。识别PMI后有再入院风险的患者对于改善预后和医院资源利用至关重要。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


