A Rare Case of Upper Eyelid Langerhans Cell Histiocytosis.
Q3 Medicine
Korean Journal of Ophthalmology : KJO
Pub Date : 2022-10-01
Epub Date: 2022-08-19
DOI:10.3341/kjo.2022.0075
引用次数: 0
Abstract
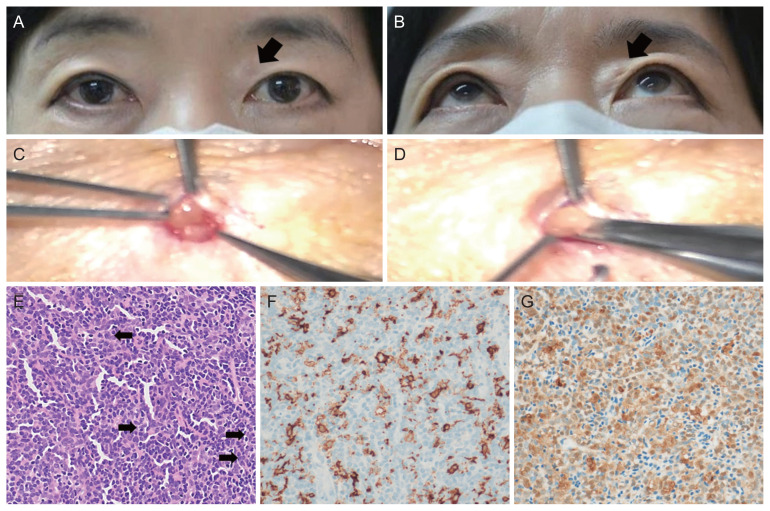
Dear Editor, Langerhans cell histiocytosis (LCH) is a rare systemic disorder characterized by clonal proliferation of histiocytes, rarer in adults than in children [1]. It can affect any organ, more frequently bones, skin, and pituitary gland [2]; however, ocular presentation of LCH has been scarcely reported. In this article, we report a rare case of eyelid LCH in an Asian adult. Informed consent for publication of the research details and clinical images was obtained from the patient. A 58-year-old Korean female patient presented with the left upper eyelid mass that gradually enlarged over a few years. She had no underlying disease. She had no history of cosmetic autologous fat transplantation or facial filler injection. Her best-corrected visual acuity was 20 / 25 in the right eye and 20 / 20 in the left eye. Intraocular pressure was in the normal range at both eyes and anterior segment was otherwise normal. Round, elevated, soft, and movable mass right beneath the skin was at the medial side of left upper eyelid (Fig. 1A, 1B). She did not have any pain or tenderness around the mass. We planned anterior orbitotomy for excisional biopsy, and the mass was excised completely from adjacent tissue (Fig. 1C, 1D). There was no postoperative complication. The gross specimen was a size of 3 mm (Fig. 1C, 1D). Microscopic photo reveals atypical histiocytic cells which contain eosinophilic cytoplasm and convoluted nuclei with groove (Fig. 1E). Immunohistochemical stain shows the histiocytic cells reactive to CD1a and anti-S100 protein (Fig. 1F, 1G). She was diagnosed as LCH based on the immunohistochemistry results and referred to oncology department for thorough evaluation to find other LCH lesions. Laboratory tests including complete blood count, blood chemistry, coagulation studies and thyroid function test, urine analysis, high resolution computed tomography and positron emission tomography were done. Since there was no other organ involvement found, treatment has been completed with the surgery and there has been no recurrence or other organ involvement in the 1-year follow-up period. In LCH patients, wide range of symptoms can appear depending on the organ involved, and it makes the diagnosis of LCH easily missed [2]. LCH is categorized as single-system or multisystem LCH depending on the number of organ involvement [3]. Symptoms can range from skin rash, simple mass, bony lesion with or without pain, diabetes to fatal problems, such as dyspnea or neurological problems [2]. Diagnosis of LCH is based on microscopic examination and at least one of the following immunological staining: langerin (CD207) positivity, CD1a positivity, and Birbeck granules on electronic microscopy [2]. S100 protein is the optional immunohistochemical study, because CD1a and langerin stain is more specific [4]. Once the diagnosis of LCH is confirmed, involvement of other organs should be evaluated [2]. The laboratory tests to be performed include a complete blood count, blood chemistry, coagulation studies, thyroid function test, and urine analysis [2]. A skeletal survey such as skull series and chest X-ray can be the first radiographic examinations to find osseous lesion [2]. Positron emission tomography can find lesions missed by other modalities [2]. Treatment recommendations are based on the extent of the organ involvement [3]. Only for solitary skin lesion without any other organ involvement, is surgical excision enough for treatment. [3]. However, in multisystem or single-system LCH with multifocal bone lesions, systemic therapy is strongly recommended [3]. No standard regimen in systemic therapy has been made but a combination of vinblastine and prednisolone therapy could serve as the standard option [3]. The prognosis of LCH is related the quantity of affected organs [5]. In conclusion, we report a rare case of LCH of the eyelid. For the patient with painless mass in the eyelid, LCH can be considered and excisional biopsy for diagnosis is mandatory. For LCH patient, consultation with oncology Korean J Ophthalmol 2022;36(5):466-467 https://doi.org/10.3341/kjo.2022.0075
罕见上眼睑朗格汉斯细胞组织细胞增多症1例。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


