Mayur Virarkar, Janio Szklaruk, Radwan Diab, Roland Bassett, Priya Bhosale
{"title":"Diagnostic value of 3.0 T versus 1.5 T MRI in staging prostate cancer: systematic review and meta-analysis.","authors":"Mayur Virarkar, Janio Szklaruk, Radwan Diab, Roland Bassett, Priya Bhosale","doi":"10.5114/pjr.2022.118685","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To compare the diagnostic performance of 3.0 T and 1.5 T MRI in the staging of prostate cancer.</p><p><strong>Material and methods: </strong>English-language studies on the diagnostic accuracy of 3.0 T and 1.5 T MRI in prostate cancer staging published through May 2020 were searched for in relevant databases. The focus was on studies in which both 3.0 T and 1.5 T MRI were performed in the study population, to reduce interstudy heterogeneity. Pooled sensitivity, specificity, diagnostic odds ratio (DOR), and area under the receiver operating characteristic curve were determined for 3.0 T and for 1.5 T along with 95% confidence intervals (CIs).</p><p><strong>Results: </strong>Out of 8 studies identified, 4 met the inclusion criteria. 3.0 T (<i>n</i> = 160) had a pooled sensitivity of 69.5% (95% CI: 56.4-80.1%) and a pooled specificity of 48.8% (95% CI: 6.0-93.4%), while 1.5 T (<i>n</i> = 139) had a pooled sensitivity of 70.6% (95% CI: 55.0-82.5%; <i>p</i> = 0.91) and a pooled specificity of 41.7% (95% CI: 6.2-88.6%; <i>p</i> = 0.88). The pooled DOR for 3.0 T was 3 (95% CI: 0-26.0%), while the pooled DOR for 1.5 T was 2 (95% CI: 0-18.0%), which was not a significant difference (<i>p</i> = 0.89).</p><p><strong>Conclusions: </strong>3.0 T has slightly better diagnostic performance than 1.5 T MRI in prostate cancer staging (3 vs. 2), although without statistical significance. Our findings suggest the need for larger, randomized trials directly comparing 3.0 T and 1.5 T MRI in prostate cancer.</p>","PeriodicalId":47128,"journal":{"name":"Polish Journal of Radiology","volume":" ","pages":"e421-e429"},"PeriodicalIF":1.6000,"publicationDate":"2022-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/26/86/PJR-87-47621.PMC9373864.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Polish Journal of Radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pjr.2022.118685","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 3
Abstract
Purpose: To compare the diagnostic performance of 3.0 T and 1.5 T MRI in the staging of prostate cancer.
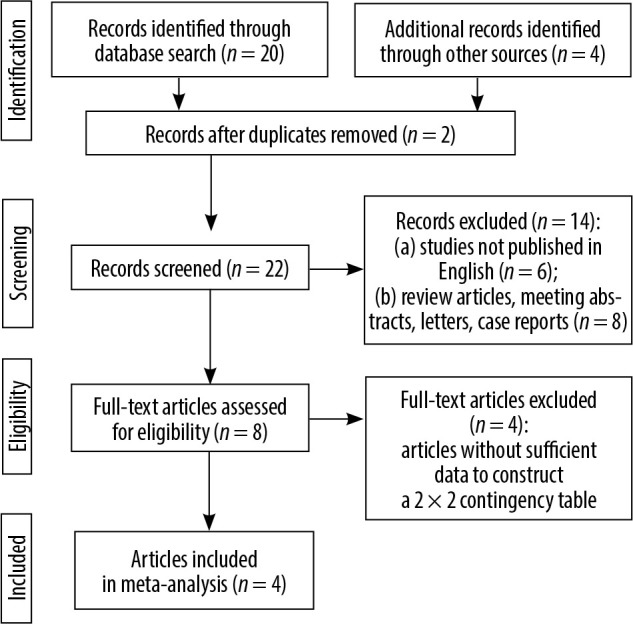
Material and methods: English-language studies on the diagnostic accuracy of 3.0 T and 1.5 T MRI in prostate cancer staging published through May 2020 were searched for in relevant databases. The focus was on studies in which both 3.0 T and 1.5 T MRI were performed in the study population, to reduce interstudy heterogeneity. Pooled sensitivity, specificity, diagnostic odds ratio (DOR), and area under the receiver operating characteristic curve were determined for 3.0 T and for 1.5 T along with 95% confidence intervals (CIs).
Results: Out of 8 studies identified, 4 met the inclusion criteria. 3.0 T (n = 160) had a pooled sensitivity of 69.5% (95% CI: 56.4-80.1%) and a pooled specificity of 48.8% (95% CI: 6.0-93.4%), while 1.5 T (n = 139) had a pooled sensitivity of 70.6% (95% CI: 55.0-82.5%; p = 0.91) and a pooled specificity of 41.7% (95% CI: 6.2-88.6%; p = 0.88). The pooled DOR for 3.0 T was 3 (95% CI: 0-26.0%), while the pooled DOR for 1.5 T was 2 (95% CI: 0-18.0%), which was not a significant difference (p = 0.89).
Conclusions: 3.0 T has slightly better diagnostic performance than 1.5 T MRI in prostate cancer staging (3 vs. 2), although without statistical significance. Our findings suggest the need for larger, randomized trials directly comparing 3.0 T and 1.5 T MRI in prostate cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


