{"title":"A Surgical Case of Bow Hunter's Syndrome Diagnosed by Cervical Rotational MRA.","authors":"Hidenori Matsuoka, So Ohashi, Michihisa Narikiyo, Ryo Nogami, Keita Hashimoto, Hirokazu Nagasaki, Yoshifumi Tsuboi","doi":"10.1155/2022/6091597","DOIUrl":null,"url":null,"abstract":"<p><p>Bow hunter's syndrome is an ischemic manifestation of vertebrobasilar artery (VA) insufficiency due to stenosis or occlusion of the contralateral VA at the bony elements of the atlas and axis during neck rotation. In early reports, VA stenosis at the craniovertebral junction was the main cause, but later, symptoms due to VA occlusion at the middle and lower cervical vertebrae were also included in this pathology. Although the confirmed diagnosis is usually determined by dynamic digital subtraction angiography (DSA), we have experienced a method of minimally invasive MR angiogram (MRA) that provides the same diagnostic value as DSA and would like to present it here. The patient was a 61-year-old man who had been visiting the outpatient clinic for cervical spondylosis due to neck pain for 9 months. When he rotated his neck to the left side, dizziness and syncope appeared. Initial MRA in the neutral position did not show any steno-occlusive changes in the vertebrobasilar artery. In our hospital, repeated MRA with the neck rotated 45 degrees to the left demonstrated ipsilateral left VA severe stenosis. Subsequent DSA showed the same findings, with occlusion of the left VA. CT of the cervical spine revealed a ventral C3/4 osteophyte within the foramen. Based on these findings, instability at the C3-4 during head rotation was considered the cause of the vertebrobasilar insufficiency. The patient underwent anterior discectomy and fusion (ACDF) at the C3/4 level using a cylindrical titanium cage. Immediately after the surgery, the patient's symptoms improved dramatically and did not appear even when the neck were fully rotated to the left. More than 5 years have passed since the surgery, and the patient is still in good health.</p>","PeriodicalId":30287,"journal":{"name":"Case Reports in Orthopedics","volume":" ","pages":"6091597"},"PeriodicalIF":0.6000,"publicationDate":"2022-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9371809/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/6091597","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 1
Abstract
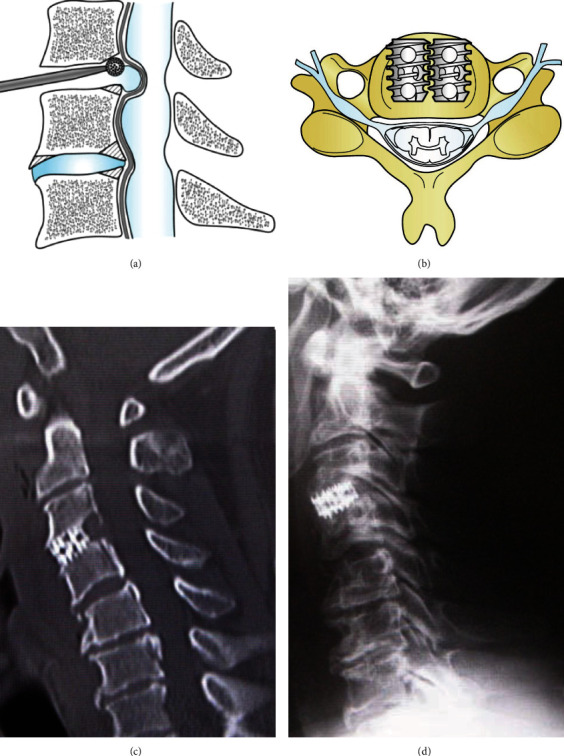
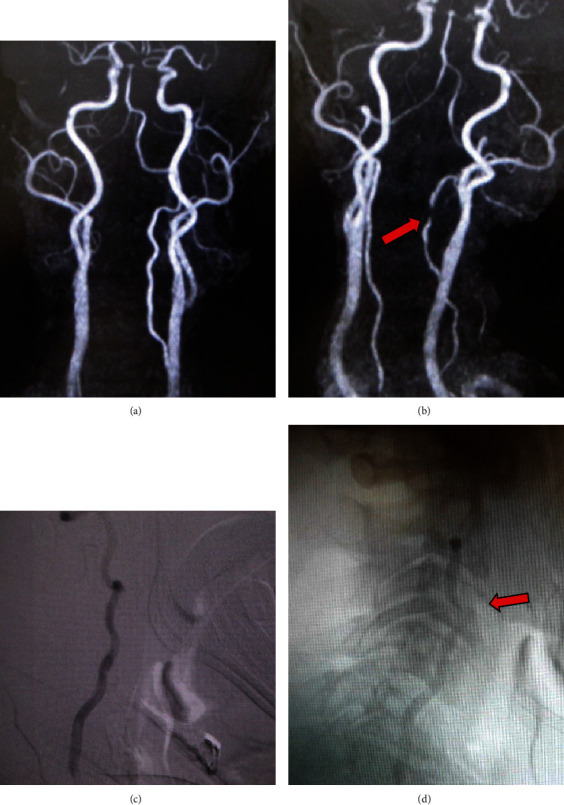
Bow hunter's syndrome is an ischemic manifestation of vertebrobasilar artery (VA) insufficiency due to stenosis or occlusion of the contralateral VA at the bony elements of the atlas and axis during neck rotation. In early reports, VA stenosis at the craniovertebral junction was the main cause, but later, symptoms due to VA occlusion at the middle and lower cervical vertebrae were also included in this pathology. Although the confirmed diagnosis is usually determined by dynamic digital subtraction angiography (DSA), we have experienced a method of minimally invasive MR angiogram (MRA) that provides the same diagnostic value as DSA and would like to present it here. The patient was a 61-year-old man who had been visiting the outpatient clinic for cervical spondylosis due to neck pain for 9 months. When he rotated his neck to the left side, dizziness and syncope appeared. Initial MRA in the neutral position did not show any steno-occlusive changes in the vertebrobasilar artery. In our hospital, repeated MRA with the neck rotated 45 degrees to the left demonstrated ipsilateral left VA severe stenosis. Subsequent DSA showed the same findings, with occlusion of the left VA. CT of the cervical spine revealed a ventral C3/4 osteophyte within the foramen. Based on these findings, instability at the C3-4 during head rotation was considered the cause of the vertebrobasilar insufficiency. The patient underwent anterior discectomy and fusion (ACDF) at the C3/4 level using a cylindrical titanium cage. Immediately after the surgery, the patient's symptoms improved dramatically and did not appear even when the neck were fully rotated to the left. More than 5 years have passed since the surgery, and the patient is still in good health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


