Paul C Mullan, Christopher M Pruitt, Kelly A Levasseur, Charles G Macias, Raina Paul, Holly Depinet, Anh Thy H Nguyen, Elliot Melendez
{"title":"Intravenous Fluid Bolus Rates Associated with Outcomes in Pediatric Sepsis: A Multi-Center Analysis.","authors":"Paul C Mullan, Christopher M Pruitt, Kelly A Levasseur, Charles G Macias, Raina Paul, Holly Depinet, Anh Thy H Nguyen, Elliot Melendez","doi":"10.2147/OAEM.S368442","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Pediatric sepsis guidelines recommend rapid intravenous fluid (IVF) bolus administration rates (BAR). Recent sepsis studies suggest that rapid BAR may be associated with increased morbidity. We aimed to describe the association between emergency department (ED) IVF BAR and clinical outcomes in pediatric sepsis.</p><p><strong>Patients and methods: </strong>Secondary post-hoc analysis of retrospective cohort data from 19 hospitals in the Pediatric Septic Shock Collaborative (PSSC) database. Patients with presumed septic shock were defined by severe sepsis/septic shock diagnostic codes, receipt of septic shock therapies, or floor-to-ICU transfers within 12 hours from ED admission for septic shock. Patients (2 months-21 years) with complete data on weight, antibiotic receipt, bolus timing, and bolus volumes were included. The primary outcome was 30-day mortality. Associations between BAR and mortality and secondary (intubation or non-invasive positive pressure ventilation = NIPPV) outcomes were assessed using unadjusted and adjusted logistic regression.</p><p><strong>Results: </strong>The PSSC database included 6731 patients; 3969 met inclusion and received a median ED volume of 40.2 mL/kg. Seventy-six (1.9%) patients died, 151 (3.8%) were intubated, and 235 (5.9%) had NIPPV administered. The median BAR was 25.7 mL/kg/hr. For each 20 mL/kg/hr increase in BAR, the adjusted odds ratio (aOR) for 30-day mortality [aOR = 1.11 (95% CI 1.01, 1.23)], intubation [aOR = 1.25 (95% CI 1.09, 1.44)], and NIPPV [aOR = 1.20 (95% CI 1.05, 1.38)] significantly increased.</p><p><strong>Conclusion: </strong>Faster ED IVF bolus administration rates in this pediatric sepsis database were associated with higher adjusted odds of death, intubation and NIPPV. Controlled trials are needed to determine if these associations are replicable.</p>","PeriodicalId":503614,"journal":{"name":"Open Access Emergency Medicine : OAEM","volume":" ","pages":"375-384"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/32/44/oaem-14-375.PMC9342868.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine : OAEM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S368442","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Purpose: Pediatric sepsis guidelines recommend rapid intravenous fluid (IVF) bolus administration rates (BAR). Recent sepsis studies suggest that rapid BAR may be associated with increased morbidity. We aimed to describe the association between emergency department (ED) IVF BAR and clinical outcomes in pediatric sepsis.
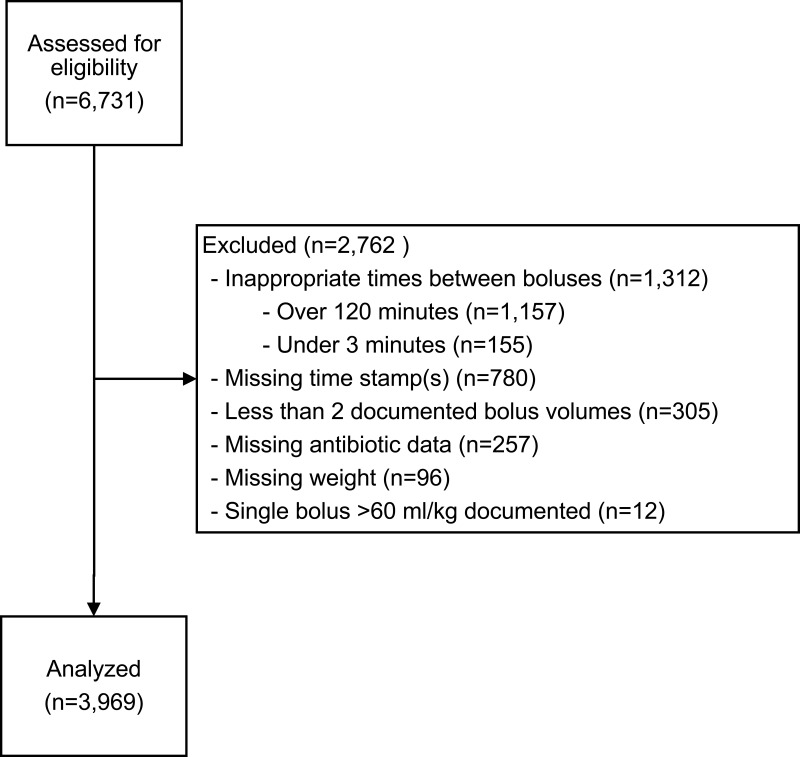
Patients and methods: Secondary post-hoc analysis of retrospective cohort data from 19 hospitals in the Pediatric Septic Shock Collaborative (PSSC) database. Patients with presumed septic shock were defined by severe sepsis/septic shock diagnostic codes, receipt of septic shock therapies, or floor-to-ICU transfers within 12 hours from ED admission for septic shock. Patients (2 months-21 years) with complete data on weight, antibiotic receipt, bolus timing, and bolus volumes were included. The primary outcome was 30-day mortality. Associations between BAR and mortality and secondary (intubation or non-invasive positive pressure ventilation = NIPPV) outcomes were assessed using unadjusted and adjusted logistic regression.
Results: The PSSC database included 6731 patients; 3969 met inclusion and received a median ED volume of 40.2 mL/kg. Seventy-six (1.9%) patients died, 151 (3.8%) were intubated, and 235 (5.9%) had NIPPV administered. The median BAR was 25.7 mL/kg/hr. For each 20 mL/kg/hr increase in BAR, the adjusted odds ratio (aOR) for 30-day mortality [aOR = 1.11 (95% CI 1.01, 1.23)], intubation [aOR = 1.25 (95% CI 1.09, 1.44)], and NIPPV [aOR = 1.20 (95% CI 1.05, 1.38)] significantly increased.
Conclusion: Faster ED IVF bolus administration rates in this pediatric sepsis database were associated with higher adjusted odds of death, intubation and NIPPV. Controlled trials are needed to determine if these associations are replicable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


