Increased Right Ventricular Pressure as a Predictor of Acute Decompensated Heart Failure in End-Stage Renal Disease Patients on Maintenance Hemodialysis.
Bong-Joon Kim, Soo-Jin Kim, Sung-Il Im, Hyun-Su Kim, Jung-Ho Heo, Ho Sik Shin, Ye Na Kim, Yeonsoon Jung, Hark Rim
{"title":"Increased Right Ventricular Pressure as a Predictor of Acute Decompensated Heart Failure in End-Stage Renal Disease Patients on Maintenance Hemodialysis.","authors":"Bong-Joon Kim, Soo-Jin Kim, Sung-Il Im, Hyun-Su Kim, Jung-Ho Heo, Ho Sik Shin, Ye Na Kim, Yeonsoon Jung, Hark Rim","doi":"10.36628/ijhf.2022.0001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Many patients with end-stage renal disease (ESRD) on hemodialysis (HD) have reduced vascular compliance and are likely to develop heart failure (HF). This study aimed to determine the factors associated with acute decompensation events among ESRD patients undergoing HD.</p><p><strong>Methods: </strong>We retrospectively investigated ESRD patients on HD using a medical record review. We divided the patients into those admitted to hospital due to acute decompensated heart failure (ADHF) and those who were not. We compared the medical histories, electrocardiograms, and echocardiographic and laboratory data between the two groups.</p><p><strong>Results: </strong>Of the 188 ESRD patients on HD, 87 were excluded, and 101 were enrolled (mean age: 63.7 years; 52.1% male). Thirty patients (29.7%) were admitted due to ADHF. These patients exhibited similar left ventricular ejection fraction (LVEF), left ventricular (LV) mass index, and E/E' values compared to the non-ADHF group. However, the ADHF group exhibited significantly higher tricuspid regurgitation (TR) jet velocity (2.9±0.6 vs. 2.5±0.4 m/s; p=0.004) and right ventricular systolic pressure (RVSP) (43.5±17.2 vs. 34.2±9.9 mmHg; p=0.009) than the non-ADHF group, respectively. A multivariate logistic regression analysis demonstrated that the TR jet velocity (odds ratio, 8.356; 95% confidence interval, 1.806-38.658; p=0.007) was an independent predictor of ADHF after adjusting for age and sex, while the LVEF and E/E' were not.</p><p><strong>Conclusions: </strong>Our data showed that an increased TR jet velocity was an independent predictor of ADHF events in ESRD patients on HD, but the LVEF and E/E' were not.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"4 3","pages":"154-162"},"PeriodicalIF":0.0000,"publicationDate":"2022-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b7/cb/ijhf-4-154.PMC9383351.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2022.0001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
Background and objectives: Many patients with end-stage renal disease (ESRD) on hemodialysis (HD) have reduced vascular compliance and are likely to develop heart failure (HF). This study aimed to determine the factors associated with acute decompensation events among ESRD patients undergoing HD.
Methods: We retrospectively investigated ESRD patients on HD using a medical record review. We divided the patients into those admitted to hospital due to acute decompensated heart failure (ADHF) and those who were not. We compared the medical histories, electrocardiograms, and echocardiographic and laboratory data between the two groups.
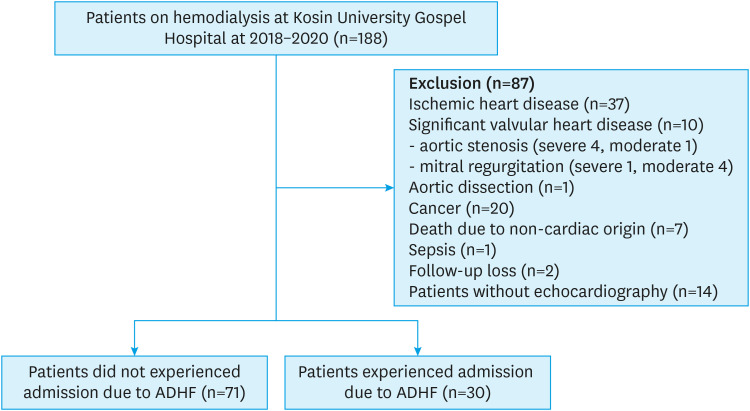
Results: Of the 188 ESRD patients on HD, 87 were excluded, and 101 were enrolled (mean age: 63.7 years; 52.1% male). Thirty patients (29.7%) were admitted due to ADHF. These patients exhibited similar left ventricular ejection fraction (LVEF), left ventricular (LV) mass index, and E/E' values compared to the non-ADHF group. However, the ADHF group exhibited significantly higher tricuspid regurgitation (TR) jet velocity (2.9±0.6 vs. 2.5±0.4 m/s; p=0.004) and right ventricular systolic pressure (RVSP) (43.5±17.2 vs. 34.2±9.9 mmHg; p=0.009) than the non-ADHF group, respectively. A multivariate logistic regression analysis demonstrated that the TR jet velocity (odds ratio, 8.356; 95% confidence interval, 1.806-38.658; p=0.007) was an independent predictor of ADHF after adjusting for age and sex, while the LVEF and E/E' were not.
Conclusions: Our data showed that an increased TR jet velocity was an independent predictor of ADHF events in ESRD patients on HD, but the LVEF and E/E' were not.
背景和目的:许多接受血液透析(HD)的终末期肾病(ESRD)患者血管顺应性降低,并可能发展为心力衰竭(HF)。本研究旨在确定与接受HD的ESRD患者急性失代偿事件相关的因素。方法:我们使用病历回顾对患有HD的ESRD患者进行回顾性调查。我们将患者分为因急性失代偿性心力衰竭(ADHF)住院的患者和非急性失代偿性心力衰竭住院的患者。我们比较了两组患者的病史、心电图、超声心动图和实验室数据。结果:188例合并HD的ESRD患者中,87例被排除,101例入组(平均年龄:63.7岁;52.1%的男性)。30例(29.7%)因ADHF入院。与非adhf组相比,这些患者表现出相似的左室射血分数(LVEF)、左室质量指数(LV)和E/E’值。ADHF组三尖瓣反流(TR)射流速度显著高于ADHF组(2.9±0.6 vs. 2.5±0.4 m/s);p=0.004)和右心室收缩压(RVSP)(43.5±17.2∶34.2±9.9 mmHg;p=0.009)高于非adhf组。多因素logistic回归分析表明,TR射流速度(优势比为8.356;95%置信区间为1.806-38.658;p=0.007)是年龄和性别调整后ADHF的独立预测因子,而LVEF和E/E′则不是。结论:我们的数据显示,TR射流速度的增加是HD的ESRD患者ADHF事件的独立预测因子,但LVEF和E/E'不是。



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


