{"title":"Scoring systems in critically ill: Which one to use in cancer patients?","authors":"Anisha Beniwal, Deven Juneja, Omender Singh, Amit Goel, Akhilesh Singh, Hemant Kumar Beniwal","doi":"10.5492/wjccm.v11.i6.364","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Scoring systems have not been evaluated in oncology patients. We aimed to assess the performance of Acute Physiology and Chronic Health Evaluation (APACHE) II, APACHE III, APACHE IV, Simplified Acute Physiology Score (SAPS) II, SAPS III, Mortality Probability Model (MPM) II<sub>0</sub> and Sequential Organ Failure Assessment (SOFA) score in critically ill oncology patients.</p><p><strong>Aim: </strong>To compare the efficacy of seven commonly employed scoring systems to predict outcomes of critically ill cancer patients.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 400 consecutive cancer patients admitted in the medical intensive care unit over a two-year period. Primary outcome was hospital mortality and the secondary outcome measure was comparison of various scoring systems in predicting hospital mortality.</p><p><strong>Results: </strong>In our study, the overall intensive care unit and hospital mortality was 43.5% and 57.8%, respectively. All of the seven tested scores underestimated mortality. The mortality as predicted by MPM II<sub>0</sub> predicted death rate (PDR) was nearest to the actual mortality followed by that predicted by APACHE II, with a standardized mortality rate (SMR) of 1.305 and 1.547, respectively. The best calibration was shown by the APACHE III score (<i>χ</i> <sup>2</sup> = 4.704, <i>P</i> = 0.788). On the other hand, SOFA score (<i>χ</i> <sup>2</sup> = 15.966, <i>P</i> = 0.025) had the worst calibration, although the difference was not statistically significant. All of the seven scores had acceptable discrimination with good efficacy however, SAPS III PDR and MPM II<sub>0</sub> PDR (AUROC = 0.762), had a better performance as compared to others. The correlation between the different scoring systems was significant (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>All the severity scores were tested under-predicted mortality in the present study. As the difference in efficacy and performance was not statistically significant, the choice of scoring system used may depend on the ease of use and local preferences.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"11 6","pages":"364-374"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/36/WJCCM-11-364.PMC9693908.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5492/wjccm.v11.i6.364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Scoring systems have not been evaluated in oncology patients. We aimed to assess the performance of Acute Physiology and Chronic Health Evaluation (APACHE) II, APACHE III, APACHE IV, Simplified Acute Physiology Score (SAPS) II, SAPS III, Mortality Probability Model (MPM) II0 and Sequential Organ Failure Assessment (SOFA) score in critically ill oncology patients.
Aim: To compare the efficacy of seven commonly employed scoring systems to predict outcomes of critically ill cancer patients.
Methods: We conducted a retrospective analysis of 400 consecutive cancer patients admitted in the medical intensive care unit over a two-year period. Primary outcome was hospital mortality and the secondary outcome measure was comparison of various scoring systems in predicting hospital mortality.
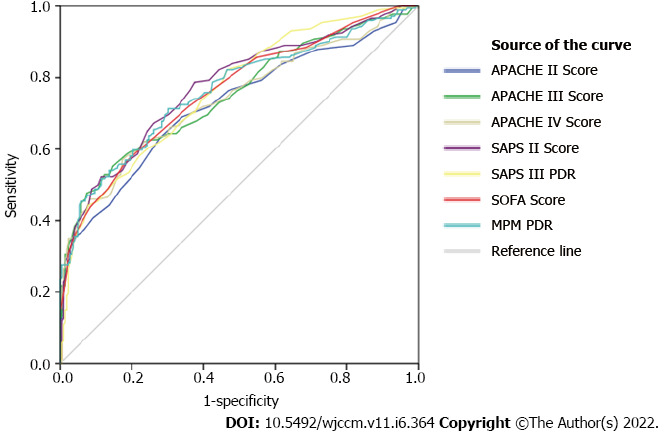
Results: In our study, the overall intensive care unit and hospital mortality was 43.5% and 57.8%, respectively. All of the seven tested scores underestimated mortality. The mortality as predicted by MPM II0 predicted death rate (PDR) was nearest to the actual mortality followed by that predicted by APACHE II, with a standardized mortality rate (SMR) of 1.305 and 1.547, respectively. The best calibration was shown by the APACHE III score (χ2 = 4.704, P = 0.788). On the other hand, SOFA score (χ2 = 15.966, P = 0.025) had the worst calibration, although the difference was not statistically significant. All of the seven scores had acceptable discrimination with good efficacy however, SAPS III PDR and MPM II0 PDR (AUROC = 0.762), had a better performance as compared to others. The correlation between the different scoring systems was significant (P < 0.001).
Conclusion: All the severity scores were tested under-predicted mortality in the present study. As the difference in efficacy and performance was not statistically significant, the choice of scoring system used may depend on the ease of use and local preferences.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


