Hye-Mee Kwon, Jae Hwan Kim, Ji-Young Kim, Gyu-Sam Hwang
{"title":"Five-year all-cause mortality in critically ill liver transplant patients with coronary artery disease: analysis of acute-on chronic liver failure.","authors":"Hye-Mee Kwon, Jae Hwan Kim, Ji-Young Kim, Gyu-Sam Hwang","doi":"10.17085/apm.22168","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with acute-on-chronic liver failure (ACLF) are critically ill and have high waiting-list mortality. Although studies demonstrated that appropriately treated coronary artery disease (CAD) should not be regarded as a contraindication to liver transplant (LT), data regarding long-term outcomes in critically ill liver LT recipients are lacking. The aim of this study was to compare the rates of all-cause death at 5 years following LT in patients with ACLF with or without CAD.</p><p><strong>Methods: </strong>Between 2010 and 2020, we evaluated 921 consecutive LT patients (MELD score, 32 ± 9) and ACLF classified by CLIF-C ACLF score. Up to 5-year all-cause death according to the CAD status was examined. CAD was defined as a preoperative history of coronary artery bypass graft or a percutaneous intervention and old myocardial infarction. Kaplan-Meier survival analysis was used.</p><p><strong>Results: </strong>Up to 5 years, 212 (23.0%) of all ACLF patients (n = 921) in whom 17 (29.3%) of 58 CAD patients died. In patients with CAD (6.3%, 58/921), the Kaplan-Meier cumulative mortality rate at 5 years was numerically higher but was not statistically significant when compared with those without CAD (32.9% vs. 23.5%, log-rank, P = 0.25). In subgr oup analysis, there were comparable risks of cumulative mortalities at 5 years across the stratification of ACLF grade 1, 2, and 3 (log-rank P = 0.062, P = 0.72, and P = 0.999, respectively).</p><p><strong>Conclusions: </strong>All-cause mortality is high in patients with ACLF after LT but is not related to the presence of revascularized or treated CAD, across the stratification of ACLF grades.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":" ","pages":"412-419"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/31/apm-22168.PMC9663955.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.22168","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Patients with acute-on-chronic liver failure (ACLF) are critically ill and have high waiting-list mortality. Although studies demonstrated that appropriately treated coronary artery disease (CAD) should not be regarded as a contraindication to liver transplant (LT), data regarding long-term outcomes in critically ill liver LT recipients are lacking. The aim of this study was to compare the rates of all-cause death at 5 years following LT in patients with ACLF with or without CAD.
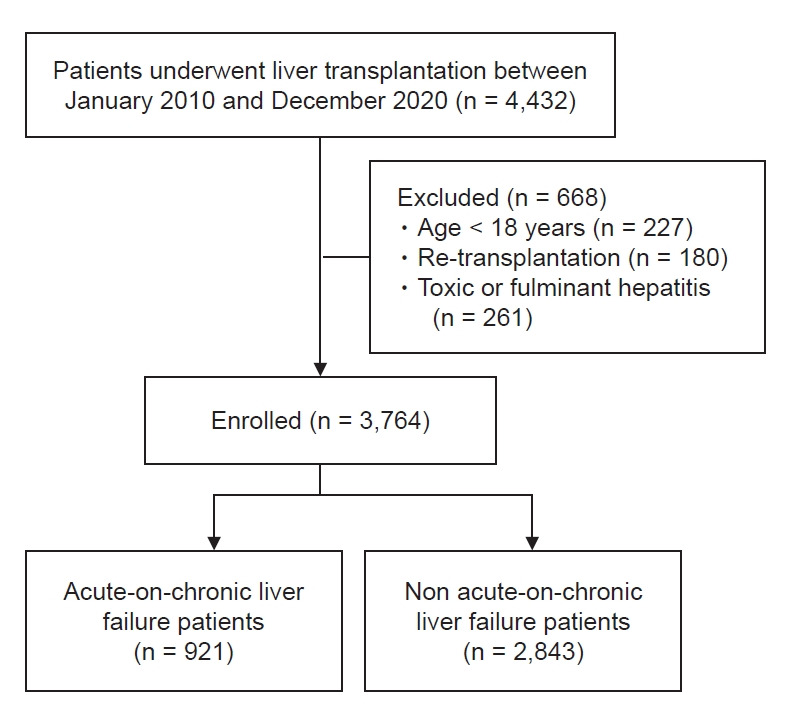
Methods: Between 2010 and 2020, we evaluated 921 consecutive LT patients (MELD score, 32 ± 9) and ACLF classified by CLIF-C ACLF score. Up to 5-year all-cause death according to the CAD status was examined. CAD was defined as a preoperative history of coronary artery bypass graft or a percutaneous intervention and old myocardial infarction. Kaplan-Meier survival analysis was used.
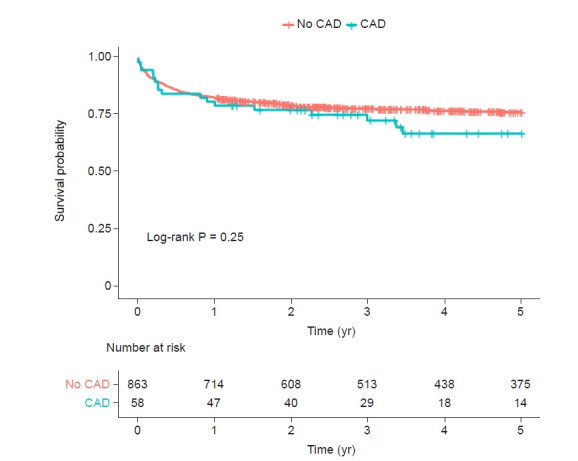
Results: Up to 5 years, 212 (23.0%) of all ACLF patients (n = 921) in whom 17 (29.3%) of 58 CAD patients died. In patients with CAD (6.3%, 58/921), the Kaplan-Meier cumulative mortality rate at 5 years was numerically higher but was not statistically significant when compared with those without CAD (32.9% vs. 23.5%, log-rank, P = 0.25). In subgr oup analysis, there were comparable risks of cumulative mortalities at 5 years across the stratification of ACLF grade 1, 2, and 3 (log-rank P = 0.062, P = 0.72, and P = 0.999, respectively).
Conclusions: All-cause mortality is high in patients with ACLF after LT but is not related to the presence of revascularized or treated CAD, across the stratification of ACLF grades.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


