Postrenal acute kidney injury from a sliding inguinal hernia.
CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne
Pub Date : 2022-08-22
DOI:10.1503/cmaj.211805
引用次数: 0
Abstract
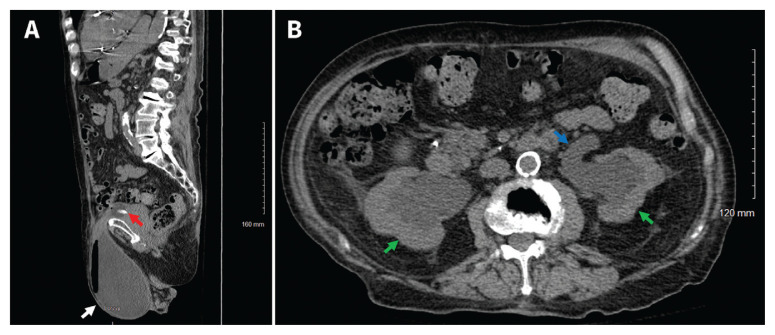
CMAJ | August 22, 2022 | Volume 194 | Issue 32 © 2022 CMA Impact Inc. or its licensors A 92-year-old man with chronic kidney disease (baseline creatinine 120 μmol/L) developed acute kidney injury (highest creatinine 422 μmol/L) while hospitalized following his third myocardial infarction. He had no pain or lower urinary tract symptoms, but had noticed a bulge in his left inguinal area for the previous 2 years. Physical examination showed that the patient was frail, with a large, partially reducible, left inguinal mass. His acute kidney injury did not resolve after intravenous hydration. We ordered pelvic ultrasonography, which showed moderate-to-severe bilateral hydronephrosis and a poorly visualized left testicle. We inserted a Foley catheter and consulted a urologist. We ordered computed tomography to look for intrinsic and extrinsic causes of the hydronephrosis, which showed that most of the bladder had herniated through a left inguinal hernia. It also showed bilateral hydronephrosis and hydroureter (Figure 1). We attempted a mechanical reduction of the bladder hernia, which was not successful. We offered the patient and his family surgical repair or more conservative management. Because of his high surgical risk, they chose nonoperative management. We inserted bilateral nephrostomy tubes, and the acute kidney injury improved. We subsequently removed the tubes and discharged the patient with an indwelling Foley catheter. He did not have further complications related to his hernia or his urinary system during the 6 months after discharge. Bladder hernias are uncommon, accounting for 1%–4% of inguinal hernias.1 Only 7%–10% are diagnosed preoperatively.1,2 Inguinal bladder hernias presenting as obstructive uropathy are infrequent, but should be considered in patients with an inguinal mass and concomitant acute kidney injury based on history and physical examination.2 The diagnosis can be confirmed with ultrasonography, computed tomography or cystography.1 Patients who are at low-to-moderate operative risk are usually offered surgery, but decompression with transient nephrostomy tubes and a permanent bladder catheter is an alternative for patients who have a high operative risk. References
腹股沟滑动疝所致肾后急性肾损伤。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

自引率
0.00%
发文量
0
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


