Ranjita Misra, Samantha Shawley-Brzoska, Raihan Khan, Brenna O Kirk, Sijin Wen, Usha Sambamoorthi
{"title":"Addressing Diabetes Distress in Self-Management Programs: Results of a Randomized Feasibility Study.","authors":"Ranjita Misra, Samantha Shawley-Brzoska, Raihan Khan, Brenna O Kirk, Sijin Wen, Usha Sambamoorthi","doi":"10.13023/jah.0303.06","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>West Virginia ranks 1st nationally in the prevalence of hypertension (HTN; 43.8%) and diabetes (16.2%). Patients with type 2 diabetes mellitus (T2DM) are distressed over physical and psychological burden of disease self-management.</p><p><strong>Methods: </strong>This study investigated the effectiveness of an intervention to reduce diabetes distress and outcomes [glycemic control, blood pressure (BP)] among T2DM adults with comorbid HTN. Participants were randomized to a 12-week diabetes and hypertension self-management program versus a 3-month wait-listed control group. Trained health coaches and experts implemented the lifestyle program in a faith-based setting using an adapted evidence-based curriculum. Twenty adults with T2DM and HTN (n=10 per group) completed baseline and 12-week assessments. Diabetes distress was measured by using a validated Diabetes Distress Survey (17-item Likert scale; four sub-scales of emotional burden, physician related burden, regimen related burden, and interpersonal distress). Baseline and post-intervention changes in diabetes distress were compared for both groups; reduction in distress in the intervention groups are depicted using waterfall plots. The mean age, HbA1c and BMI were 55 ± 9.6 years, 7.8 ± 2.24 and 36.4 ± 8.8, respectively. Diabetes distress (total; mean) was 1.84±0.71.</p><p><strong>Results: </strong>Participants reported higher diabetes distress related to emotional burden (2.1±0.94) and regimen-related distress (2.0 ± 0.74); physician-related distress was the lowest (1.18±0.64). In general, diabetes distress reduced among intervention participants and was especially significant among those with HbA1c ≤ 8% (r=0.28, p=0.4), and systolic/diastolic BP ≤140/80 mm Hg (r=0.045, P=0.18).</p><p><strong>Implications: </strong>Findings suggest that lifestyle self-management programs have the potential to reduce diabetes distress.</p>","PeriodicalId":73599,"journal":{"name":"Journal of Appalachian health","volume":" ","pages":"68-85"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9192112/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Appalachian health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13023/jah.0303.06","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: West Virginia ranks 1st nationally in the prevalence of hypertension (HTN; 43.8%) and diabetes (16.2%). Patients with type 2 diabetes mellitus (T2DM) are distressed over physical and psychological burden of disease self-management.
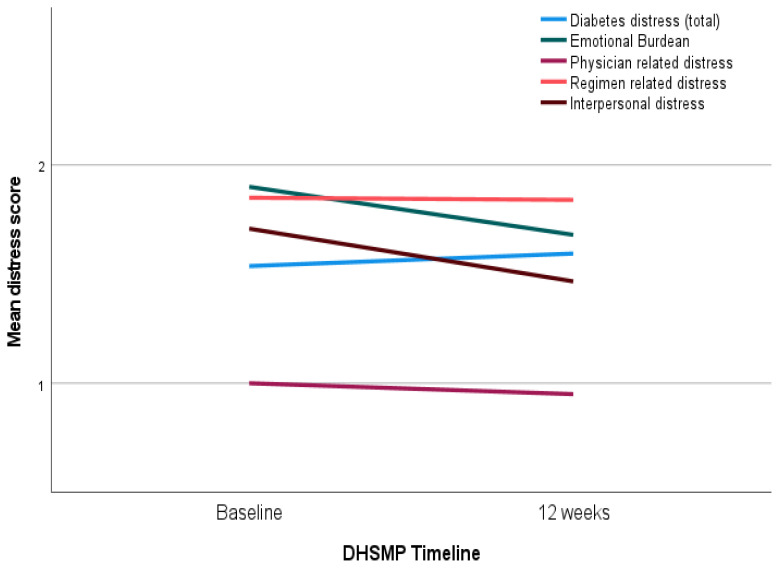
Methods: This study investigated the effectiveness of an intervention to reduce diabetes distress and outcomes [glycemic control, blood pressure (BP)] among T2DM adults with comorbid HTN. Participants were randomized to a 12-week diabetes and hypertension self-management program versus a 3-month wait-listed control group. Trained health coaches and experts implemented the lifestyle program in a faith-based setting using an adapted evidence-based curriculum. Twenty adults with T2DM and HTN (n=10 per group) completed baseline and 12-week assessments. Diabetes distress was measured by using a validated Diabetes Distress Survey (17-item Likert scale; four sub-scales of emotional burden, physician related burden, regimen related burden, and interpersonal distress). Baseline and post-intervention changes in diabetes distress were compared for both groups; reduction in distress in the intervention groups are depicted using waterfall plots. The mean age, HbA1c and BMI were 55 ± 9.6 years, 7.8 ± 2.24 and 36.4 ± 8.8, respectively. Diabetes distress (total; mean) was 1.84±0.71.
Results: Participants reported higher diabetes distress related to emotional burden (2.1±0.94) and regimen-related distress (2.0 ± 0.74); physician-related distress was the lowest (1.18±0.64). In general, diabetes distress reduced among intervention participants and was especially significant among those with HbA1c ≤ 8% (r=0.28, p=0.4), and systolic/diastolic BP ≤140/80 mm Hg (r=0.045, P=0.18).
Implications: Findings suggest that lifestyle self-management programs have the potential to reduce diabetes distress.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


