{"title":"Donor-derived diffuse large B-cell lymphoma after haploidentical stem cell transplantation for acute myeloid leukemia.","authors":"Anna Kawashiri, Shun-Ichiro Nakagawa, Chisato Ishiguro, Kanako Mochizuki, Yoshinobu Maeda, Toshiro Kurokawa","doi":"10.3960/jslrt.22014","DOIUrl":null,"url":null,"abstract":"<p><p>We report a case of donor-derived diffuse large B-cell lymphoma (DLBCL), which developed 5 years after stem cell transplantation from a human leukocyte antigen (HLA)-haploidentical donor for acute myeloid leukemia (AML). A 51-year-old male was diagnosed with AML with variant KMT2A translocation involving t(6;11)(q13;q23). After 12 cycles of azacitidine treatment, fluorescence in situ hybridization (FISH) for KMT2A split signal indicated that 94% of his bone marrow (BM) cells were positive. He underwent peripheral blood stem cell transplantation (PBSCT) from his HLA-haploidentical son. The preconditioning regimen consisted of fludarabine, busulfan, melphalan, and antithymocyte globulin (ATG). The graft-versus-host disease (GVHD) prophylaxis consisted of tacrolimus and short-term methotrexate. On day 28, KMT2A FISH analysis indicated that he had achieved a complete response (CR). He continued to receive tacrolimus for the limited type of cutaneous chronic GVHD. Five years after the transplantation, positron emission tomography/computed tomography (PET/CT) showed an abdominal tumor. The tumor was diagnosed as DLBCL without Epstein-Barr virus. BM aspiration revealed the infiltration of lymphoma cells with t(8;14)(q24;q32). Chimerism analysis showed that both the peripheral blood (PB) and abdominal lymphoma cells were of donor origin. After 4 cycles of salvage chemotherapy, PET/CT showed that a CR had been achieved. He underwent a second PBSCT from an HLA-identical unrelated donor. The preconditioning regimen and GVHD prophylaxis were the same as those for the first PBSCT without ATG. The patient's PB revealed complete second donor-type chimerism, and the patient has maintained a CR since the second transplantation.</p>","PeriodicalId":520662,"journal":{"name":"Journal of clinical and experimental hematopathology : JCEH","volume":" ","pages":"175-180"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/3e/jslrt-62-175.PMC9635034.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical and experimental hematopathology : JCEH","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.22014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
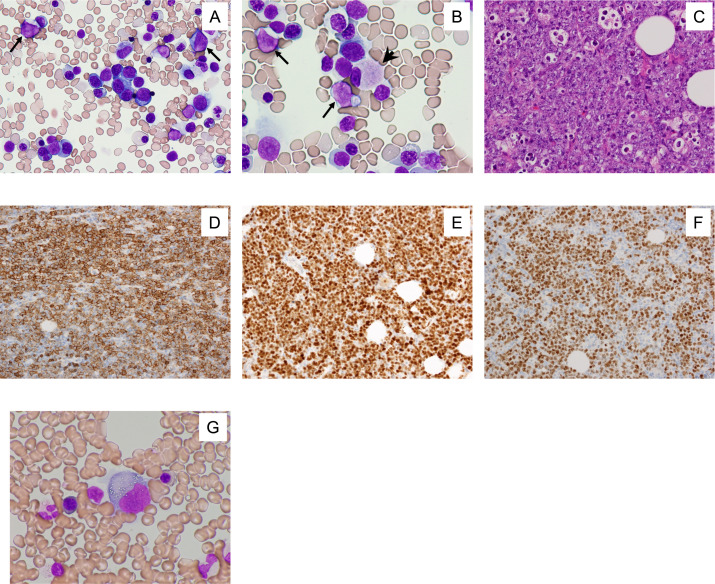
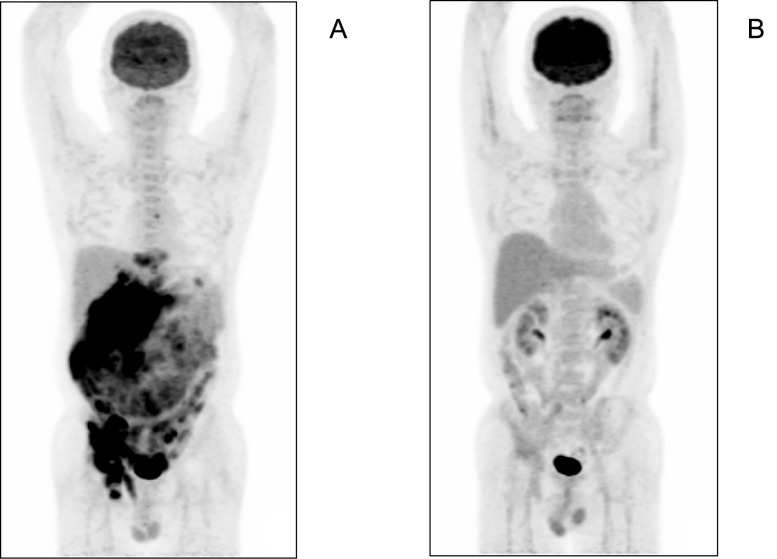
We report a case of donor-derived diffuse large B-cell lymphoma (DLBCL), which developed 5 years after stem cell transplantation from a human leukocyte antigen (HLA)-haploidentical donor for acute myeloid leukemia (AML). A 51-year-old male was diagnosed with AML with variant KMT2A translocation involving t(6;11)(q13;q23). After 12 cycles of azacitidine treatment, fluorescence in situ hybridization (FISH) for KMT2A split signal indicated that 94% of his bone marrow (BM) cells were positive. He underwent peripheral blood stem cell transplantation (PBSCT) from his HLA-haploidentical son. The preconditioning regimen consisted of fludarabine, busulfan, melphalan, and antithymocyte globulin (ATG). The graft-versus-host disease (GVHD) prophylaxis consisted of tacrolimus and short-term methotrexate. On day 28, KMT2A FISH analysis indicated that he had achieved a complete response (CR). He continued to receive tacrolimus for the limited type of cutaneous chronic GVHD. Five years after the transplantation, positron emission tomography/computed tomography (PET/CT) showed an abdominal tumor. The tumor was diagnosed as DLBCL without Epstein-Barr virus. BM aspiration revealed the infiltration of lymphoma cells with t(8;14)(q24;q32). Chimerism analysis showed that both the peripheral blood (PB) and abdominal lymphoma cells were of donor origin. After 4 cycles of salvage chemotherapy, PET/CT showed that a CR had been achieved. He underwent a second PBSCT from an HLA-identical unrelated donor. The preconditioning regimen and GVHD prophylaxis were the same as those for the first PBSCT without ATG. The patient's PB revealed complete second donor-type chimerism, and the patient has maintained a CR since the second transplantation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


