Raelina S Howell, Margret S Magid, Keith A Kuenzler, T K Susheel Kumar
{"title":"Giant mediastinal teratoma in a young infant: a case report.","authors":"Raelina S Howell, Margret S Magid, Keith A Kuenzler, T K Susheel Kumar","doi":"10.21037/med-21-45","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Giant mediastinal tumors in the pediatric population can pose unique challenges for resection such as cardiovascular collapse on induction of anesthesia and injury to surrounding structures that may be compressed, displaced, or invaded by the mass. Principles that must be borne in mind during removal of giant mediastinal masses include: appropriate cross-sectional imaging to define extent of mass; airway control during induction of anesthesia; a multidisciplinary collaborative approach including cardiothoracic surgery; preparation for urgent sternotomy; plan for peripheral cannulation to institute cardiopulmonary bypass if needed; preservation of neurovasculature structures during dissection; complete resection whenever possible. While complete resection is desirable and results in an excellent prognosis, it may not be achievable especially if the tumor encases coronary arteries, and it is acceptable to leave small amounts of tumor behind.</p><p><strong>Case description: </strong>Here we present a case describing surgical management of a giant mediastinal teratoma in a two-month-old female. The patient was found to have a large mediastinal mass during workup for cough and noisy breathing. She underwent preoperative echocardiogram demonstrating normal cardiac function followed by uncomplicated, open resection of the mass.</p><p><strong>Conclusions: </strong>Giant mediastinal tumors give rise to unique challenges for resection in small infants. The principles of airway control, preparation for urgent sternotomy, preparation for peripheral cardiopulmonary bypass cannulation, and preservation of neurovasculature during dissection must be borne in mind.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":" ","pages":"25"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/55/9c/med-06-25.PMC9385876.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-21-45","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
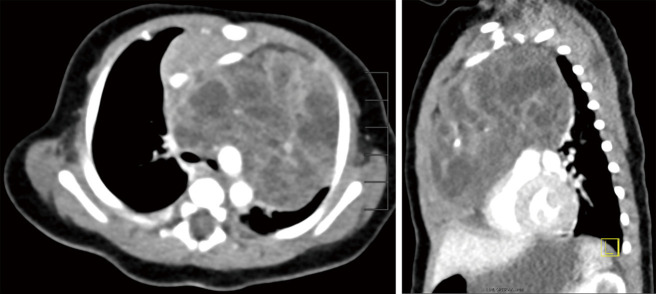
Background: Giant mediastinal tumors in the pediatric population can pose unique challenges for resection such as cardiovascular collapse on induction of anesthesia and injury to surrounding structures that may be compressed, displaced, or invaded by the mass. Principles that must be borne in mind during removal of giant mediastinal masses include: appropriate cross-sectional imaging to define extent of mass; airway control during induction of anesthesia; a multidisciplinary collaborative approach including cardiothoracic surgery; preparation for urgent sternotomy; plan for peripheral cannulation to institute cardiopulmonary bypass if needed; preservation of neurovasculature structures during dissection; complete resection whenever possible. While complete resection is desirable and results in an excellent prognosis, it may not be achievable especially if the tumor encases coronary arteries, and it is acceptable to leave small amounts of tumor behind.
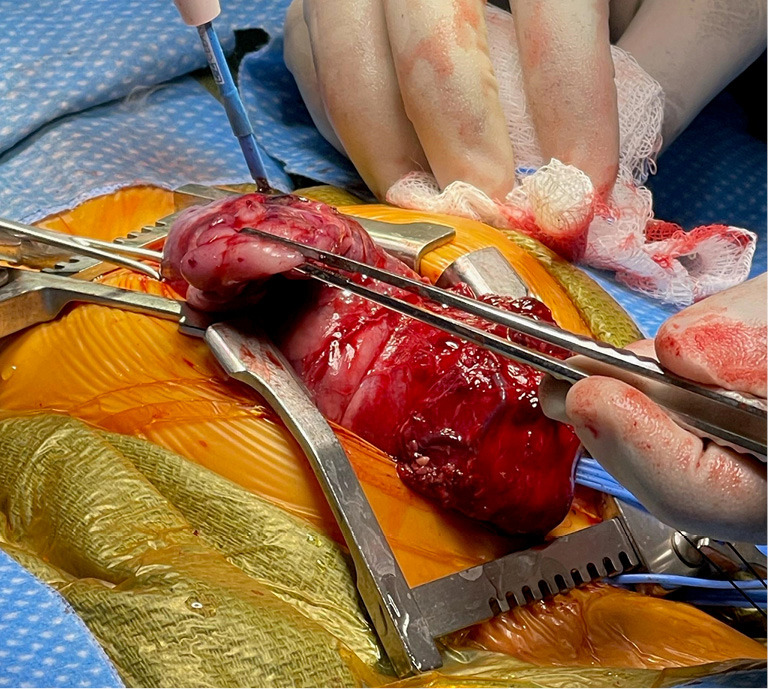
Case description: Here we present a case describing surgical management of a giant mediastinal teratoma in a two-month-old female. The patient was found to have a large mediastinal mass during workup for cough and noisy breathing. She underwent preoperative echocardiogram demonstrating normal cardiac function followed by uncomplicated, open resection of the mass.
Conclusions: Giant mediastinal tumors give rise to unique challenges for resection in small infants. The principles of airway control, preparation for urgent sternotomy, preparation for peripheral cardiopulmonary bypass cannulation, and preservation of neurovasculature during dissection must be borne in mind.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


