Pressley A Chakales, Max C Herman, Ling Chen Chien, Spencer K Hutto
{"title":"Pachymeningitis in Biopsy-Proven Sarcoidosis: Clinical Course, Radiographic Findings, Response to Treatment, and Long-term Outcomes.","authors":"Pressley A Chakales, Max C Herman, Ling Chen Chien, Spencer K Hutto","doi":"10.1212/NXI.0000000000200028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Meningeal inflammation is one of the most common manifestations of neurosarcoidosis, occurring in 16%-69% of affected patients. While the clinical and radiographic features of leptomeningitis in neurosarcoidosis are well known, those of pachymeningitis are far less clear. Our primary aim was to study the clinicoradiographic features of pachymeningeal involvement in neurosarcoidosis and its evolution over time in response to treatment.</p><p><strong>Methods: </strong>Patients with a diagnosis of neurosarcoidosis seen at Emory University (January 2011-August 2021) were included if pachymeningeal involvement was evident by MRI and the patient's sarcoidosis was pathologically confirmed (from a CNS or non-CNS site).</p><p><strong>Results: </strong>Twenty-six of 215 (12.1%) patients with neurosarcoidosis qualified for inclusion. Pathologic confirmation came from CNS tissue in 50%. The median age of onset was 43.5 years; most were male (16/26, 61.5%). Symptoms were primarily related to pachymeningitis in 20/26 (76.9%). Headache (19/26, 73.1%), visual dysfunction (12/26, 46.2%), and seizures (7/26, 26.9%) were the most common symptoms. All patients had cranial pachymeningitis; only a single patient undergoing spinal imaging (1/11, 9.1%) had spinal pachymeningitis. The falx cerebri (16/26, 61.5%) was the most commonly affected dural structure, but the anterior and middle cranial fossae and tentorium cerebelli were frequently involved (12/26 each, 46.2%). The pachymeningeal lesions were unifocal (11/26, 42.3%) or multifocal (15/26, 57.7%) in distribution, nodular morphologically (23/25, 92.0%), and homogeneously enhancing (24/25, 96.0%). Symptomatic improvement occurred with steroids initially in 22/25 (88.0%). Ultimately, 23/26 (88.5%) required initiation of steroid-sparing immunosuppressants, including 8/26 (30.8%) eventually undergoing TNF inhibition. Pachymeningeal relapses occurred in 7/26 (26.9%). The median clinical follow-up was 48 months. The median modified Rankin scale score at last follow-up improved to 1.0 from 2.0 at presentation.</p><p><strong>Discussion: </strong>Pachymeningitis due to sarcoidosis often presents with headaches, visual dysfunction, and seizures; it usually affects the dura of the falx cerebri, anterior and middle cranial fossae, and tentorium cerebelli and tends to require steroid-sparing immunosuppressants. It has the potential to relapse, but the prospect for recovery is good.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/61/e9/NXI-2022-200034.PMC9513981.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background and objectives: Meningeal inflammation is one of the most common manifestations of neurosarcoidosis, occurring in 16%-69% of affected patients. While the clinical and radiographic features of leptomeningitis in neurosarcoidosis are well known, those of pachymeningitis are far less clear. Our primary aim was to study the clinicoradiographic features of pachymeningeal involvement in neurosarcoidosis and its evolution over time in response to treatment.
Methods: Patients with a diagnosis of neurosarcoidosis seen at Emory University (January 2011-August 2021) were included if pachymeningeal involvement was evident by MRI and the patient's sarcoidosis was pathologically confirmed (from a CNS or non-CNS site).
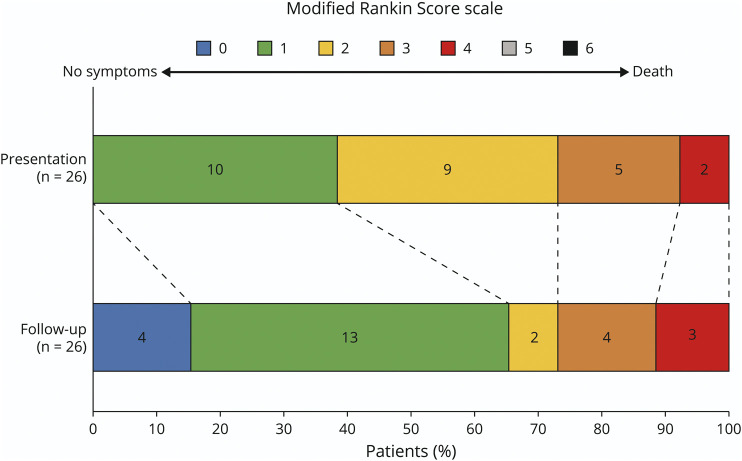
Results: Twenty-six of 215 (12.1%) patients with neurosarcoidosis qualified for inclusion. Pathologic confirmation came from CNS tissue in 50%. The median age of onset was 43.5 years; most were male (16/26, 61.5%). Symptoms were primarily related to pachymeningitis in 20/26 (76.9%). Headache (19/26, 73.1%), visual dysfunction (12/26, 46.2%), and seizures (7/26, 26.9%) were the most common symptoms. All patients had cranial pachymeningitis; only a single patient undergoing spinal imaging (1/11, 9.1%) had spinal pachymeningitis. The falx cerebri (16/26, 61.5%) was the most commonly affected dural structure, but the anterior and middle cranial fossae and tentorium cerebelli were frequently involved (12/26 each, 46.2%). The pachymeningeal lesions were unifocal (11/26, 42.3%) or multifocal (15/26, 57.7%) in distribution, nodular morphologically (23/25, 92.0%), and homogeneously enhancing (24/25, 96.0%). Symptomatic improvement occurred with steroids initially in 22/25 (88.0%). Ultimately, 23/26 (88.5%) required initiation of steroid-sparing immunosuppressants, including 8/26 (30.8%) eventually undergoing TNF inhibition. Pachymeningeal relapses occurred in 7/26 (26.9%). The median clinical follow-up was 48 months. The median modified Rankin scale score at last follow-up improved to 1.0 from 2.0 at presentation.
Discussion: Pachymeningitis due to sarcoidosis often presents with headaches, visual dysfunction, and seizures; it usually affects the dura of the falx cerebri, anterior and middle cranial fossae, and tentorium cerebelli and tends to require steroid-sparing immunosuppressants. It has the potential to relapse, but the prospect for recovery is good.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


