Chieh-Kuo Lin, Ka-I Leong, Cheng-Hung How, Hu-Lin Christina Wang, Chao-Yu Liu
{"title":"Drainless thoracoscopic surgery should be avoided in primary spontaneous pneumothorax with pleural adhesion.","authors":"Chieh-Kuo Lin, Ka-I Leong, Cheng-Hung How, Hu-Lin Christina Wang, Chao-Yu Liu","doi":"10.1093/icvts/ivac237","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Drainless thoracoscopic surgery, defined by omitting chest drain after surgery, has been demonstrated to be feasible in selected patients for pulmonary resection. However, drainless procedure for the treatment of primary spontaneous pneumothorax has raised concerns for its safety and thus has been less often reported. We aimed to share our preliminary experience regarding how to select patients with spontaneous pneumothorax for this procedure.</p><p><strong>Methods: </strong>A retrospective study recruiting 303 consecutive patients with the diagnosis of spontaneous pneumothorax undergoing thoracoscopic surgery in our centre from August 2016 to June 2020 was done. After careful selection, the chest drain was omitted in selected patients who underwent non-intubated uniportal thoracoscopic surgery. Patients' clinical characteristics and perioperative outcomes were analysed.</p><p><strong>Results: </strong>A total of 34 patients underwent drainless thoracoscopic surgery for the treatment of spontaneous pneumothorax. Pleural adhesion was noted in 9 patients during surgery, and all of them (100%) developed residual pneumothorax, among which intercostal drainage was required in 2 (22.2%) patients and ipsilateral pneumothorax recurred 3 years after surgery in 1 (11.1%) patient. Among the remaining 25 without pleural adhesion, 17 (68.0%) developed minor residual pneumothorax (P = 0.006), which all resolved spontaneously within 1-2 weeks, with no complications or recurrence during postoperative follow-up for at least 2 years.</p><p><strong>Conclusions: </strong>Drainless thoracoscopic surgery for the treatment of primary spontaneous pneumothorax is feasible but can be risky without careful patient selection. In our experience, the drainless procedure should be avoided in patients with identifiable pleural adhesion noted during surgery.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9492251/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac237","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: Drainless thoracoscopic surgery, defined by omitting chest drain after surgery, has been demonstrated to be feasible in selected patients for pulmonary resection. However, drainless procedure for the treatment of primary spontaneous pneumothorax has raised concerns for its safety and thus has been less often reported. We aimed to share our preliminary experience regarding how to select patients with spontaneous pneumothorax for this procedure.
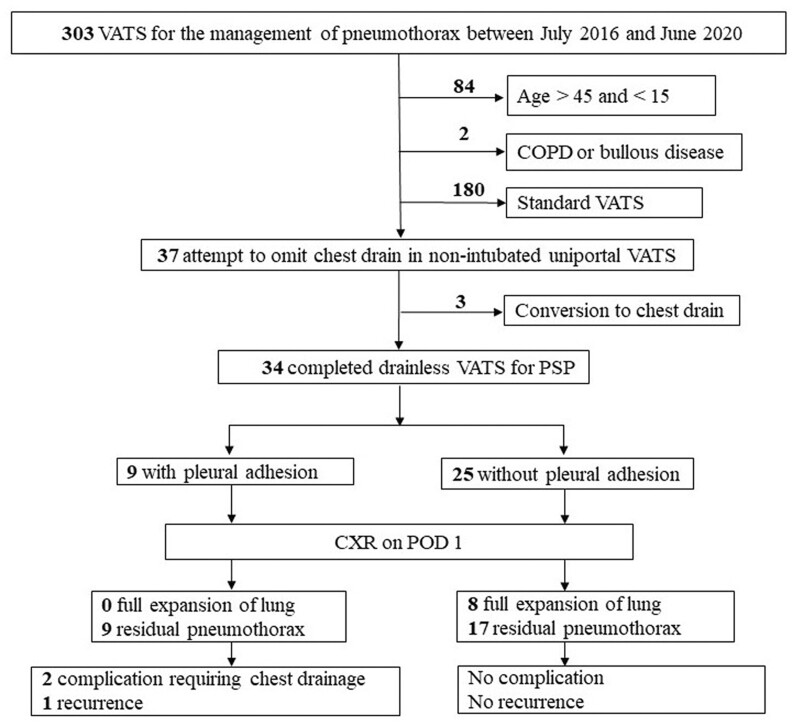
Methods: A retrospective study recruiting 303 consecutive patients with the diagnosis of spontaneous pneumothorax undergoing thoracoscopic surgery in our centre from August 2016 to June 2020 was done. After careful selection, the chest drain was omitted in selected patients who underwent non-intubated uniportal thoracoscopic surgery. Patients' clinical characteristics and perioperative outcomes were analysed.
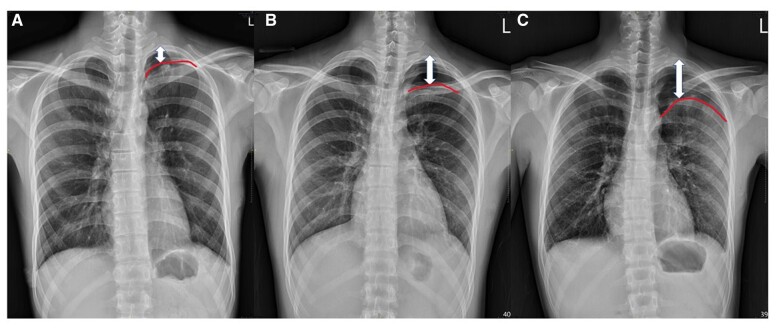
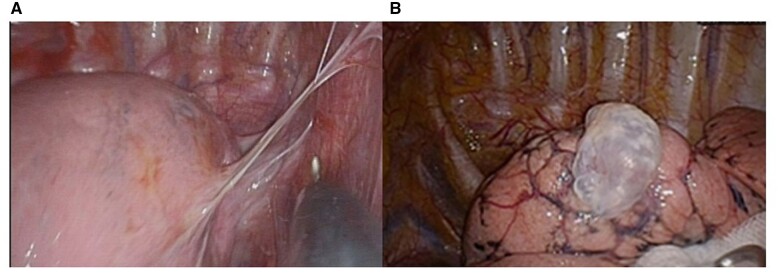
Results: A total of 34 patients underwent drainless thoracoscopic surgery for the treatment of spontaneous pneumothorax. Pleural adhesion was noted in 9 patients during surgery, and all of them (100%) developed residual pneumothorax, among which intercostal drainage was required in 2 (22.2%) patients and ipsilateral pneumothorax recurred 3 years after surgery in 1 (11.1%) patient. Among the remaining 25 without pleural adhesion, 17 (68.0%) developed minor residual pneumothorax (P = 0.006), which all resolved spontaneously within 1-2 weeks, with no complications or recurrence during postoperative follow-up for at least 2 years.
Conclusions: Drainless thoracoscopic surgery for the treatment of primary spontaneous pneumothorax is feasible but can be risky without careful patient selection. In our experience, the drainless procedure should be avoided in patients with identifiable pleural adhesion noted during surgery.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


