Vivek Satyasi, Gayatra Mainali, Jahnavi Chatterjee, Sita Paudel
{"title":"Encephalitis with Extensive Cortical Brain Magnetic Resonance Imaging Changes Secondary to Myelin Oligodendrocyte Glycoprotein Antibody Disease.","authors":"Vivek Satyasi, Gayatra Mainali, Jahnavi Chatterjee, Sita Paudel","doi":"10.12659/AJCR.936361","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND The relatively new autoimmune disorder, anti-myelin oligodendrocyte glycoprotein (MOG) disease is particularly interesting because of its broad range of presentations. This entity's appearance on magnetic resonance imaging (MRI) of the brain often makes identifying this disease a challenging process. Younger patients tend to present with an acute disseminated encephalomyelitis picture, with encephalopathy and multifocal neurological signs, while older patients are more likely to present with optic neuritis. We, however, report an atypical case of a patient who presented with encephalopathy, seizures, and significant cortical and subcortical gray matter involvement and was found to have anti-MOG positivity in serum. CASE REPORT A 17-month-old previously healthy boy presented to Emergency Department with fever, lethargy, vomiting, and left-sided weakness. Eventually, he required intubation due to a prolonged seizure. Continuous electroencephalogram captured several focal seizures, and MRI of the brain showed cortical and subcortical T2 hyperintensities. After extensive laboratory evaluation, he tested positive for anti-MOG antibody. He was empirically started on high-dose intravenous pulse methylprednisolone, followed by plasma exchange, given the poor response to the intravenous steroids. At the 5-month follow-up, the results of the neurological examination had dramatically improved, and MRI findings had largely resolved. CONCLUSIONS This case highlights the importance of suspecting anti-MOG antibody-mediated encephalitis, even while ruling out infectious etiologies, in children presenting with encephalopathy, seizures and MRI abnormalities. Prompt recognition would allow for less delay in treatment and hopefully improve prognosis.</p>","PeriodicalId":205256,"journal":{"name":"The American Journal of Case Reports","volume":" ","pages":"e936361"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c4/39/amjcaserep-23-e936361.PMC9444166.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.936361","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
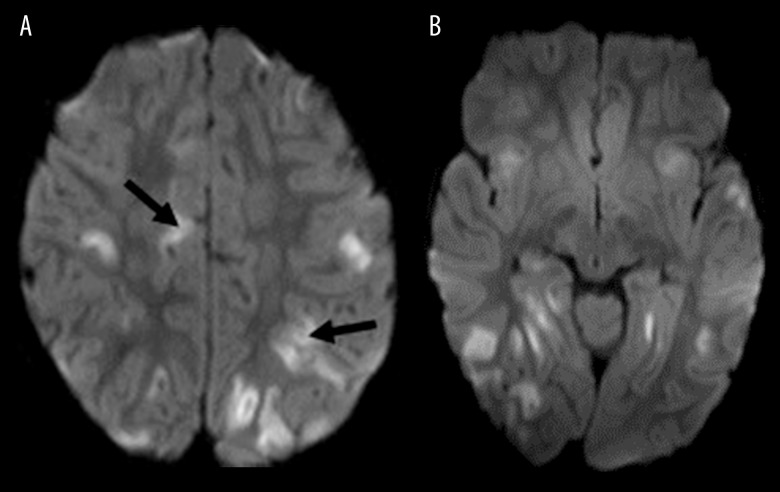
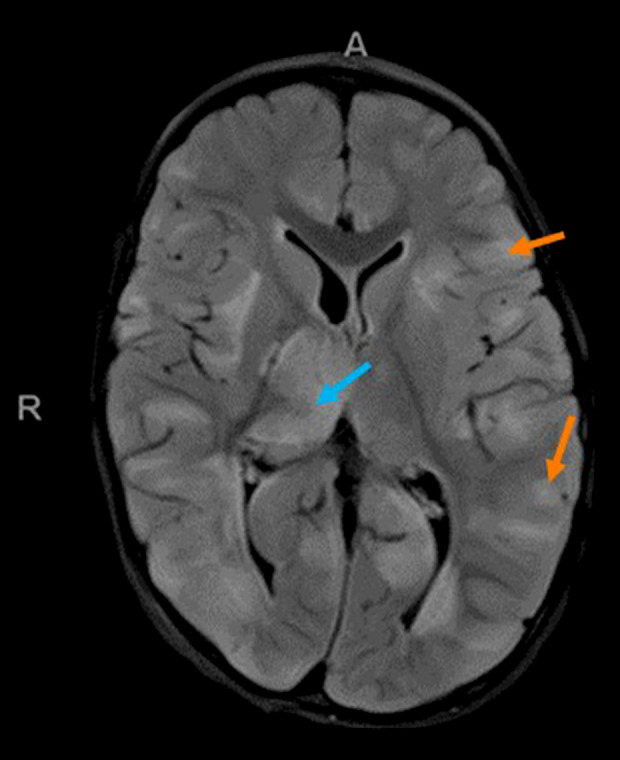
BACKGROUND The relatively new autoimmune disorder, anti-myelin oligodendrocyte glycoprotein (MOG) disease is particularly interesting because of its broad range of presentations. This entity's appearance on magnetic resonance imaging (MRI) of the brain often makes identifying this disease a challenging process. Younger patients tend to present with an acute disseminated encephalomyelitis picture, with encephalopathy and multifocal neurological signs, while older patients are more likely to present with optic neuritis. We, however, report an atypical case of a patient who presented with encephalopathy, seizures, and significant cortical and subcortical gray matter involvement and was found to have anti-MOG positivity in serum. CASE REPORT A 17-month-old previously healthy boy presented to Emergency Department with fever, lethargy, vomiting, and left-sided weakness. Eventually, he required intubation due to a prolonged seizure. Continuous electroencephalogram captured several focal seizures, and MRI of the brain showed cortical and subcortical T2 hyperintensities. After extensive laboratory evaluation, he tested positive for anti-MOG antibody. He was empirically started on high-dose intravenous pulse methylprednisolone, followed by plasma exchange, given the poor response to the intravenous steroids. At the 5-month follow-up, the results of the neurological examination had dramatically improved, and MRI findings had largely resolved. CONCLUSIONS This case highlights the importance of suspecting anti-MOG antibody-mediated encephalitis, even while ruling out infectious etiologies, in children presenting with encephalopathy, seizures and MRI abnormalities. Prompt recognition would allow for less delay in treatment and hopefully improve prognosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


