Chandrakant G Pujari, A V Lalitha, John Michael Raj, Ananya Kavilapurapu
{"title":"Epidemiology of Acute Respiratory Distress Syndrome in Pediatric Intensive Care Unit: Single-center Experience.","authors":"Chandrakant G Pujari, A V Lalitha, John Michael Raj, Ananya Kavilapurapu","doi":"10.5005/jp-journals-10071-24285","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute respiratory distress syndrome (ARDS) is characterized by dysregulated inflammation resulting in hypoxemia and respiratory failure and causes both morbidity and mortality.</p><p><strong>Objectives: </strong>To describe the clinical profile, outcome, and predictors of mortality in ARDS in children admitted to the Pediatric intensive care unit.</p><p><strong>Materials and methods: </strong>This is a single-center retrospective study conducted at a tertiary referral hospital in a 12-bed PICU involving children (1 month to 18 years) with ARDS as defined by Pediatric Acute Lung Injury Consensus Conference (PALICC) guidelines, over a period of 5 years (2016-2020). Demographic, clinical, and laboratory details at onset and during PICU stay were collected. Predictors of mortality were compared between survivors and non-survivors.</p><p><strong>Results: </strong>We identified 89 patients with ARDS. The median age at presentation was 76 months (12-124 months). The most common precipitating factor was pneumonia (66%). The majority of children (35.9%) had moderate ARDS. Overall mortality was 33% with more than half belonging to severe ARDS group (58%). On Kaplan-Meier survival curve analysis, the mean time to death was shorter in the severe ARDS group as compared to other groups. Multiorgan dysfunction was present in 46 (51.6%) of the cases. Non-survivors had higher mean pediatric logistic organ dysfunction (PELOD2) on day 1. PRISM III at admission, worsening trends of ventilator and oxygenation parameters (OI, P/F, MAP, and PEEP) independently predicted mortality after multivariate analysis.</p><p><strong>Conclusion: </strong>High PRISM score predicts poor outcome, and worsening trends of ventilator and oxygenation parameters (OI, P/F, MAP, and PEEP) are associated with mortality.</p><p><strong>How to cite this article: </strong>Pujari CG, Lalitha AV, Raj JM, Kavilapurapu A. Epidemiology of Acute Respiratory Distress Syndrome in Pediatric Intensive Care Unit: Single-center Experience. Indian J Crit Care Med 2022;26(8):949-955.</p>","PeriodicalId":520643,"journal":{"name":"Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine","volume":" ","pages":"949-955"},"PeriodicalIF":1.5000,"publicationDate":"2022-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d7/a8/ijccm-26-949.PMC9363796.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5005/jp-journals-10071-24285","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Acute respiratory distress syndrome (ARDS) is characterized by dysregulated inflammation resulting in hypoxemia and respiratory failure and causes both morbidity and mortality.
Objectives: To describe the clinical profile, outcome, and predictors of mortality in ARDS in children admitted to the Pediatric intensive care unit.
Materials and methods: This is a single-center retrospective study conducted at a tertiary referral hospital in a 12-bed PICU involving children (1 month to 18 years) with ARDS as defined by Pediatric Acute Lung Injury Consensus Conference (PALICC) guidelines, over a period of 5 years (2016-2020). Demographic, clinical, and laboratory details at onset and during PICU stay were collected. Predictors of mortality were compared between survivors and non-survivors.
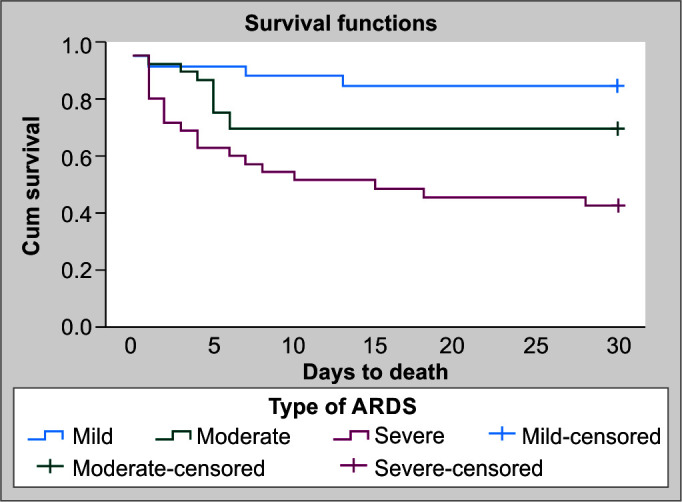
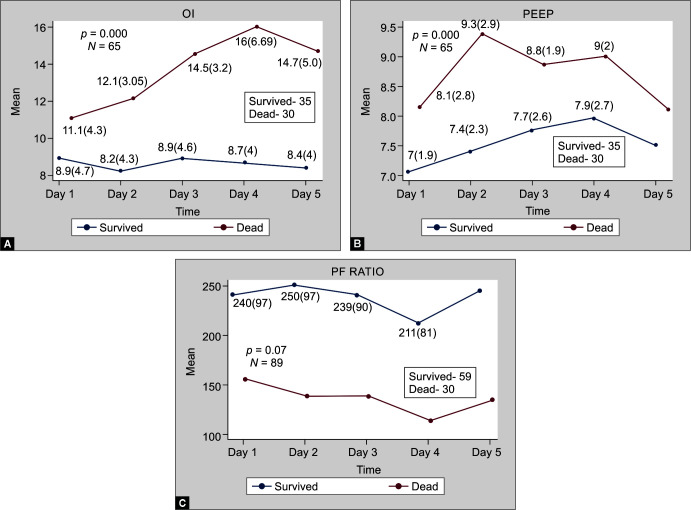
Results: We identified 89 patients with ARDS. The median age at presentation was 76 months (12-124 months). The most common precipitating factor was pneumonia (66%). The majority of children (35.9%) had moderate ARDS. Overall mortality was 33% with more than half belonging to severe ARDS group (58%). On Kaplan-Meier survival curve analysis, the mean time to death was shorter in the severe ARDS group as compared to other groups. Multiorgan dysfunction was present in 46 (51.6%) of the cases. Non-survivors had higher mean pediatric logistic organ dysfunction (PELOD2) on day 1. PRISM III at admission, worsening trends of ventilator and oxygenation parameters (OI, P/F, MAP, and PEEP) independently predicted mortality after multivariate analysis.
Conclusion: High PRISM score predicts poor outcome, and worsening trends of ventilator and oxygenation parameters (OI, P/F, MAP, and PEEP) are associated with mortality.
How to cite this article: Pujari CG, Lalitha AV, Raj JM, Kavilapurapu A. Epidemiology of Acute Respiratory Distress Syndrome in Pediatric Intensive Care Unit: Single-center Experience. Indian J Crit Care Med 2022;26(8):949-955.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


