Amber E Johnson, Shuvodra Routh, Christy N Taylor, Meagan Leopold, Kathryn Beatty, Dennis M McNamara, Esa M Davis
{"title":"Developing and Implementing an mHealth Heart Failure Self-care Program to Reduce Readmissions: Randomized Controlled Trial.","authors":"Amber E Johnson, Shuvodra Routh, Christy N Taylor, Meagan Leopold, Kathryn Beatty, Dennis M McNamara, Esa M Davis","doi":"10.2196/33286","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients admitted with decompensated heart failure (HF) are at risk for hospital readmission and poor quality of life during the discharge period. Lifestyle behavior modifications that promote the self-management of chronic cardiac diseases have been associated with an improved quality of life. However, whether a mobile health (mHealth) program can assist patients in the self-management of HF during the acute posthospital discharge period is unknown.</p><p><strong>Objective: </strong>We aimed to develop an mHealth program designed to enhance patients' self-management of HF by increasing knowledge, self-efficacy, and symptom detection. We hypothesized that patients hospitalized with HF would be willing to use a feasibly deployed mHealth program after their hospital discharge.</p><p><strong>Methods: </strong>We employed a patient-centered outcomes research methodology to design a stakeholder-informed mHealth program. Adult patients with HF admitted to a large academic hospital were enrolled and randomized to receive the mHealth intervention versus usual care. Our feasibility outcomes included ease of program deployment, use of the clinical escalation process, duration of participant recruitment, and participant attrition. Surveys assessing the demographics and clinical characteristics of HF were measured at baseline and at 30 and 90 days after discharge.</p><p><strong>Results: </strong>The study period was between July 1, 2019, and April 7, 2020. The mean cohort (N=31) age was 60.4 (range 22-85) years. Over half of the participants were men (n=18, 58%) and 77% (n=24) were White. There were no significant differences in baseline measures. We determined that an educational mHealth program tailored for patients with HF is feasibly deployed and acceptable by patients. Though not significant, we found notable trends including a higher mean quality of life at 30 days posthospitalization among program users and a longer duration before rehospitalization, which are suggestive of better HF prognosis.</p><p><strong>Conclusions: </strong>Our mHealth tool should be further assessed in a larger comparative effectiveness trial. Our pilot intervention offers promise as an innovative means to help HF patients lead healthy, independent lives. These preliminary data suggest that patient-centered mHealth tools can enable high-risk patients to play a role in the management of their HF after discharge.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT03982017; https://clinicaltrials.gov/ct2/show/NCT03982017.</p>","PeriodicalId":14706,"journal":{"name":"JMIR Cardio","volume":" ","pages":"e33286"},"PeriodicalIF":0.0000,"publicationDate":"2022-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8981015/pdf/","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cardio","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/33286","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 6
Abstract
Background: Patients admitted with decompensated heart failure (HF) are at risk for hospital readmission and poor quality of life during the discharge period. Lifestyle behavior modifications that promote the self-management of chronic cardiac diseases have been associated with an improved quality of life. However, whether a mobile health (mHealth) program can assist patients in the self-management of HF during the acute posthospital discharge period is unknown.
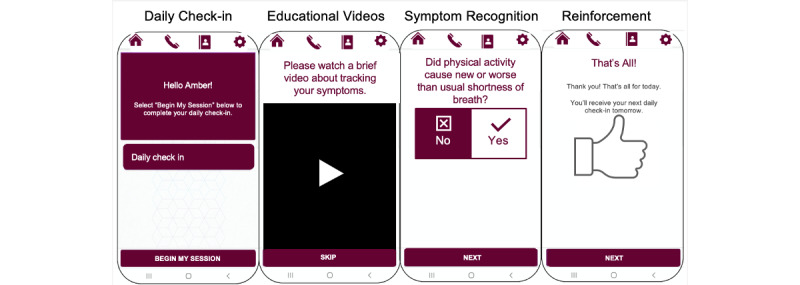
Objective: We aimed to develop an mHealth program designed to enhance patients' self-management of HF by increasing knowledge, self-efficacy, and symptom detection. We hypothesized that patients hospitalized with HF would be willing to use a feasibly deployed mHealth program after their hospital discharge.
Methods: We employed a patient-centered outcomes research methodology to design a stakeholder-informed mHealth program. Adult patients with HF admitted to a large academic hospital were enrolled and randomized to receive the mHealth intervention versus usual care. Our feasibility outcomes included ease of program deployment, use of the clinical escalation process, duration of participant recruitment, and participant attrition. Surveys assessing the demographics and clinical characteristics of HF were measured at baseline and at 30 and 90 days after discharge.
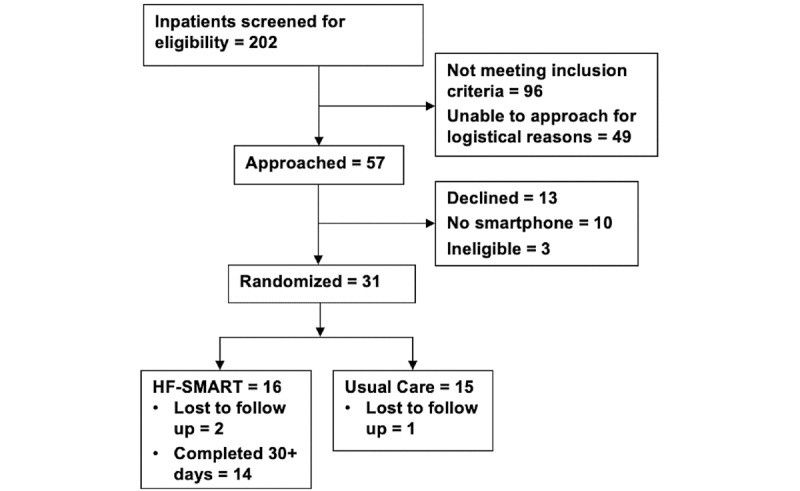
Results: The study period was between July 1, 2019, and April 7, 2020. The mean cohort (N=31) age was 60.4 (range 22-85) years. Over half of the participants were men (n=18, 58%) and 77% (n=24) were White. There were no significant differences in baseline measures. We determined that an educational mHealth program tailored for patients with HF is feasibly deployed and acceptable by patients. Though not significant, we found notable trends including a higher mean quality of life at 30 days posthospitalization among program users and a longer duration before rehospitalization, which are suggestive of better HF prognosis.
Conclusions: Our mHealth tool should be further assessed in a larger comparative effectiveness trial. Our pilot intervention offers promise as an innovative means to help HF patients lead healthy, independent lives. These preliminary data suggest that patient-centered mHealth tools can enable high-risk patients to play a role in the management of their HF after discharge.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


