Gautam Das, Vinay S Eligar, Jyothish Govindan, D Aled Rees
{"title":"Late presentation of hyperandrogenism in pregnancy: clinical features and differential diagnosis.","authors":"Gautam Das, Vinay S Eligar, Jyothish Govindan, D Aled Rees","doi":"10.1530/EDM-13-0048","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyperandrogenic states in pregnancy are rare but arise most commonly due to new-onset ovarian pathology in pregnancy. We describe the case of a young woman who presented in the latter half of her pregnancy with features of hyperandrogenism. We review the biochemical and imaging findings and discuss the differential diagnosis.</p><p><strong>Case presentation: </strong>A 26-year-old woman presented in the later part of her pregnancy with widespread hirsutism. Biochemical testing confirmed hyperandrogenism (testosterone, 13.7 nmol/l and second-trimester pregnancy range, 0.9-4.9 nmol/l), although she had no history of menstrual disturbance, hirsutism or acne prior to conception. Radiological evaluation (ultrasound and magnetic resonance imaging) revealed multiple cystic lesions in both ovaries, leading to a presumptive diagnosis of hyperreactio luteinalis (HL). The implications of maternal hyperandrogenism on foetal virilisation were considered and the patient was counselled appropriately. She delivered a healthy baby boy uneventfully. Androgen levels, hirsutism and acne normalised within a few weeks of delivery.</p><p><strong>Conclusion: </strong>HL can occur at any stage of pregnancy and is an important differential diagnosis in pregnant patients with features of androgen excess. Most cases regress spontaneously after delivery and major interventions are usually not needed.</p><p><strong>Learning points: </strong>Hyperandrogenism in pregnancy is rare.Clinical features are similar to the non-pregnant state in the mother but virilisation in the foetus can have profound consequences.HL and pregnancy luteoma are the most common ovarian pathologies leading to hyperandrogenism in pregnancy.Spontaneous regression occurs in the post-partum period in the vast majority of cases and surgery is only required for local complications.</p>","PeriodicalId":520608,"journal":{"name":"Endocrinology, diabetes & metabolism case reports","volume":" ","pages":"130048"},"PeriodicalIF":0.7000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1530/EDM-13-0048","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, diabetes & metabolism case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-13-0048","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/10/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
Background: Hyperandrogenic states in pregnancy are rare but arise most commonly due to new-onset ovarian pathology in pregnancy. We describe the case of a young woman who presented in the latter half of her pregnancy with features of hyperandrogenism. We review the biochemical and imaging findings and discuss the differential diagnosis.
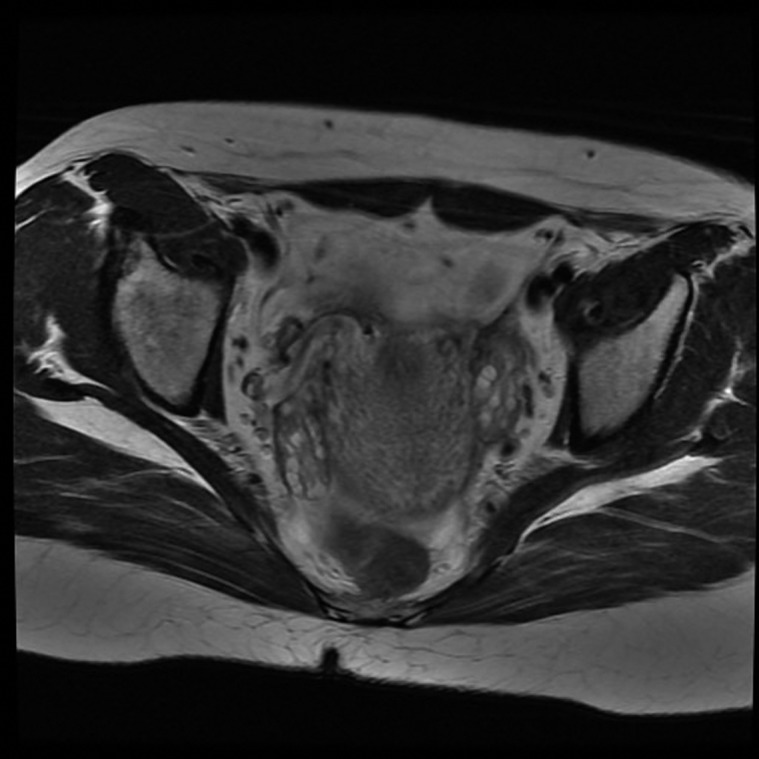
Case presentation: A 26-year-old woman presented in the later part of her pregnancy with widespread hirsutism. Biochemical testing confirmed hyperandrogenism (testosterone, 13.7 nmol/l and second-trimester pregnancy range, 0.9-4.9 nmol/l), although she had no history of menstrual disturbance, hirsutism or acne prior to conception. Radiological evaluation (ultrasound and magnetic resonance imaging) revealed multiple cystic lesions in both ovaries, leading to a presumptive diagnosis of hyperreactio luteinalis (HL). The implications of maternal hyperandrogenism on foetal virilisation were considered and the patient was counselled appropriately. She delivered a healthy baby boy uneventfully. Androgen levels, hirsutism and acne normalised within a few weeks of delivery.
Conclusion: HL can occur at any stage of pregnancy and is an important differential diagnosis in pregnant patients with features of androgen excess. Most cases regress spontaneously after delivery and major interventions are usually not needed.
Learning points: Hyperandrogenism in pregnancy is rare.Clinical features are similar to the non-pregnant state in the mother but virilisation in the foetus can have profound consequences.HL and pregnancy luteoma are the most common ovarian pathologies leading to hyperandrogenism in pregnancy.Spontaneous regression occurs in the post-partum period in the vast majority of cases and surgery is only required for local complications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


