Dominic Cavlan, Shanti Vijayaraghavan, Susan Gelding, William Drake
{"title":"GH replacement causing acute hyperglycaemia and ketonuria in a type 1 diabetic patient.","authors":"Dominic Cavlan, Shanti Vijayaraghavan, Susan Gelding, William Drake","doi":"10.1530/EDM-13-0047","DOIUrl":null,"url":null,"abstract":"<p><strong>Unlabelled: </strong>A state of insulin resistance is common to the clinical conditions of both chronic growth hormone (GH) deficiency and GH excess (acromegaly). GH has a physiological role in glucose metabolism in the acute settings of fast and exercise and is the only anabolic hormone secreted in the fasting state. We report the case of a patient in whom knowledge of this aspect of GH physiology was vital to her care. A woman with well-controlled type 1 diabetes mellitus who developed hypopituitarism following the birth of her first child required GH replacement therapy. Hours after the first dose, she developed a rapid metabolic deterioration and awoke with hyperglycaemia and ketonuria. She adjusted her insulin dose accordingly, but the pattern was repeated with each subsequent increase in her dose. Acute GH-induced lipolysis results in an abundance of free fatty acids (FFA); these directly inhibit glucose uptake into muscle, and this can lead to hyperglycaemia. This glucose-fatty acid cycle was first described by Randle et al. in 1963; it is a nutrient-mediated fine control that allows oxidative muscle to switch between glucose and fatty acids as fuel, depending on their availability. We describe the mechanism in detail.</p><p><strong>Learning points: </strong>THERE IS A COMPLEX INTERPLAY BETWEEN GH AND INSULIN RESISTANCE: chronically, both GH excess and deficiency lead to insulin resistance, but there is also an acute mechanism that is less well appreciated by clinicians.GH activates hormone-sensitive lipase to release FFA into the circulation; these may inhibit the uptake of glucose leading to hyperglycaemia and ketosis in the type 1 diabetic patient.The Randle cycle, or glucose-fatty acid cycle, outlines the mechanism for this acute relationship.Monitoring the adequacy of GH replacement in patients with type 1 diabetes is difficult, with IGF1 an unreliable marker.</p>","PeriodicalId":520608,"journal":{"name":"Endocrinology, diabetes & metabolism case reports","volume":" ","pages":"130047"},"PeriodicalIF":0.7000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3922345/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, diabetes & metabolism case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-13-0047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/9/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
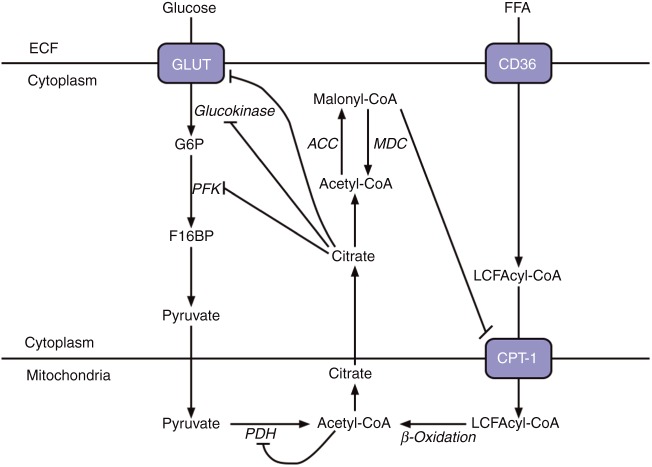
Unlabelled: A state of insulin resistance is common to the clinical conditions of both chronic growth hormone (GH) deficiency and GH excess (acromegaly). GH has a physiological role in glucose metabolism in the acute settings of fast and exercise and is the only anabolic hormone secreted in the fasting state. We report the case of a patient in whom knowledge of this aspect of GH physiology was vital to her care. A woman with well-controlled type 1 diabetes mellitus who developed hypopituitarism following the birth of her first child required GH replacement therapy. Hours after the first dose, she developed a rapid metabolic deterioration and awoke with hyperglycaemia and ketonuria. She adjusted her insulin dose accordingly, but the pattern was repeated with each subsequent increase in her dose. Acute GH-induced lipolysis results in an abundance of free fatty acids (FFA); these directly inhibit glucose uptake into muscle, and this can lead to hyperglycaemia. This glucose-fatty acid cycle was first described by Randle et al. in 1963; it is a nutrient-mediated fine control that allows oxidative muscle to switch between glucose and fatty acids as fuel, depending on their availability. We describe the mechanism in detail.
Learning points: THERE IS A COMPLEX INTERPLAY BETWEEN GH AND INSULIN RESISTANCE: chronically, both GH excess and deficiency lead to insulin resistance, but there is also an acute mechanism that is less well appreciated by clinicians.GH activates hormone-sensitive lipase to release FFA into the circulation; these may inhibit the uptake of glucose leading to hyperglycaemia and ketosis in the type 1 diabetic patient.The Randle cycle, or glucose-fatty acid cycle, outlines the mechanism for this acute relationship.Monitoring the adequacy of GH replacement in patients with type 1 diabetes is difficult, with IGF1 an unreliable marker.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


