{"title":"Delayed progression to dialysis with early and intensive management of predialysis chronic kidney disease: a case-based approach.","authors":"Stephen Thomsen","doi":"10.1159/000353265","DOIUrl":null,"url":null,"abstract":"<p><p>In addition to hypertension and diabetes, disorders in mineral metabolism and bone disease (e.g. affecting phosphorus, calcium, parathyroid hormone, and vitamin D) are common complications of chronic kidney disease (CKD) and contribute to morbidity and mortality. Consequently, CKD requires multifactorial treatment to slow CKD progression and avoid end-stage renal disease. CKD progression and treatment outcomes are monitored by measuring the estimated glomerular filtration rate (eGFR), which decreases by 2-12 ml/min/1.73 m(2) per year depending on the stage of CKD and comorbidities, such as diabetes. This paper presents representative case studies illustrating the delay and reversal of CKD progression with comprehensive, individualized treatment regimens, including non-calcium phosphate binders, antihypertensives, lipid-lowering drugs, calcimimetics, and other drugs as required, to treat each component of CKD including CKD-mineral and bone disorder. Four patients are included, with an average age of 70-81 years and CKD stage 3 or 4 accompanied by various comorbidities, most notably diabetes and hypertension. The range of treatment and follow-up durations was 6-7 years. In each case, there was evidence of slowing or prevention of CKD progression, according to eGFR and serum creatinine, regardless of the patient's age or CKD stage. Despite a baseline eGFR of <20 ml/min/1.73 m(2) in 1 female patient, after 6 years of follow-up, her eGFR had stabilized and was maintained at >15 ml/min/1.73 m(2). These observations reinforce the value of early nephrology referral and comprehensive management of CKD and underlying conditions (hypertension and diabetes) beginning at eGFR <60 ml/min/1.73 m(2). </p>","PeriodicalId":89663,"journal":{"name":"Case reports in nephrology and urology","volume":" ","pages":"74-86"},"PeriodicalIF":0.0000,"publicationDate":"2013-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000353265","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case reports in nephrology and urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000353265","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
Abstract
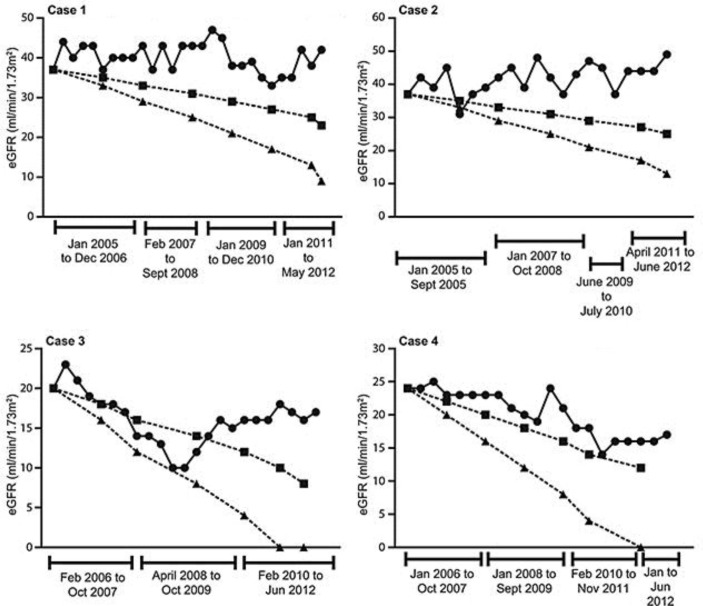
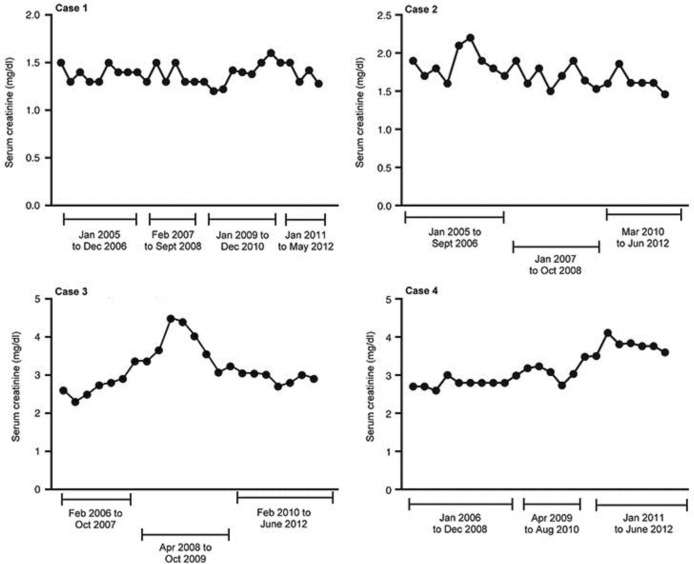
In addition to hypertension and diabetes, disorders in mineral metabolism and bone disease (e.g. affecting phosphorus, calcium, parathyroid hormone, and vitamin D) are common complications of chronic kidney disease (CKD) and contribute to morbidity and mortality. Consequently, CKD requires multifactorial treatment to slow CKD progression and avoid end-stage renal disease. CKD progression and treatment outcomes are monitored by measuring the estimated glomerular filtration rate (eGFR), which decreases by 2-12 ml/min/1.73 m(2) per year depending on the stage of CKD and comorbidities, such as diabetes. This paper presents representative case studies illustrating the delay and reversal of CKD progression with comprehensive, individualized treatment regimens, including non-calcium phosphate binders, antihypertensives, lipid-lowering drugs, calcimimetics, and other drugs as required, to treat each component of CKD including CKD-mineral and bone disorder. Four patients are included, with an average age of 70-81 years and CKD stage 3 or 4 accompanied by various comorbidities, most notably diabetes and hypertension. The range of treatment and follow-up durations was 6-7 years. In each case, there was evidence of slowing or prevention of CKD progression, according to eGFR and serum creatinine, regardless of the patient's age or CKD stage. Despite a baseline eGFR of <20 ml/min/1.73 m(2) in 1 female patient, after 6 years of follow-up, her eGFR had stabilized and was maintained at >15 ml/min/1.73 m(2). These observations reinforce the value of early nephrology referral and comprehensive management of CKD and underlying conditions (hypertension and diabetes) beginning at eGFR <60 ml/min/1.73 m(2).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


