The impact of coronary artery bypass grafting added to aortic valve replacement on long-term outcomes in octogenarian patients: a reconstructed time-to-event meta-analysis.
Alan Gallingani, Stefano D'Alessandro, Gurmeet Singh, Daniel Hernandez-Vaquero, Mevlüt Çelik, Evelina Ceccato, Francesco Nicolini, Francesco Formica
{"title":"The impact of coronary artery bypass grafting added to aortic valve replacement on long-term outcomes in octogenarian patients: a reconstructed time-to-event meta-analysis.","authors":"Alan Gallingani, Stefano D'Alessandro, Gurmeet Singh, Daniel Hernandez-Vaquero, Mevlüt Çelik, Evelina Ceccato, Francesco Nicolini, Francesco Formica","doi":"10.1093/icvts/ivac164","DOIUrl":null,"url":null,"abstract":"<p><p>The long-term results in studies comparing octogenarian patients who received either isolated surgical aortic valve replacement (i-SAVR) or coronary artery bypass grafting (CABG) in addition to SAVR are still debated. We performed a reconstructed time-to-event data meta-analysis of studies comparing i-SAVR and CABG+SAVR to evaluate the impact of CABG and to analyse the time-varying effects on long-term outcome. We performed a systematic review of the literature from January 2000 through November 2021, including studies comparing i-SAVR and CABG+SAVR, which reported at least 3-year follow-up and that plotted Kaplan-Meier curves of overall survival. The primary endpoint was overall long-term survival; secondary endpoints were in-hospital/30-day mortality and postoperative outcomes. The pooled hazard ratio (HR) and odds ratio) with 95% confidence interval (CI) were calculated for primary and secondary endpoints, respectively. Random-effect model was used in all analyses. Sixteen retrospective studies were included (5382 patients, i-SAVR = 2568 and CABG+SAVR = 2814). I-SAVR showed a lower incidence of in-hospital mortality compared to CABG+SAVR (odds ratio = 0.73; 95% CI= 0.60-0.89; P = 0.002). Landmark analyses showed a significantly higher all-cause mortality within 1 year from surgery in CABG+SAVR (HR = 1.17; 95% CI = 1.01-1.36; P = 0.03); after 1 year, no significant difference was observed (HR = 0.95; 95% CI = 0.87-1.04; P = 0.35). Landmark analysis was confirmed by time-varying trend of HR. Late survival of octogenarians did not differ significantly between the 2 interventions. Interestingly, CABG added to SAVR was associated with both higher in-hospital and within 1-year mortality after surgery, whereas this difference was statistically non-significant at long-term follow-up.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9272063/pdf/","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac164","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 7
Abstract
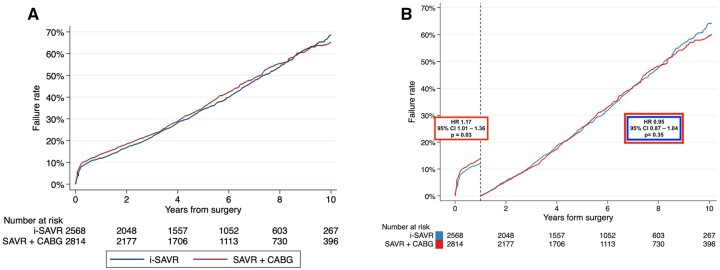
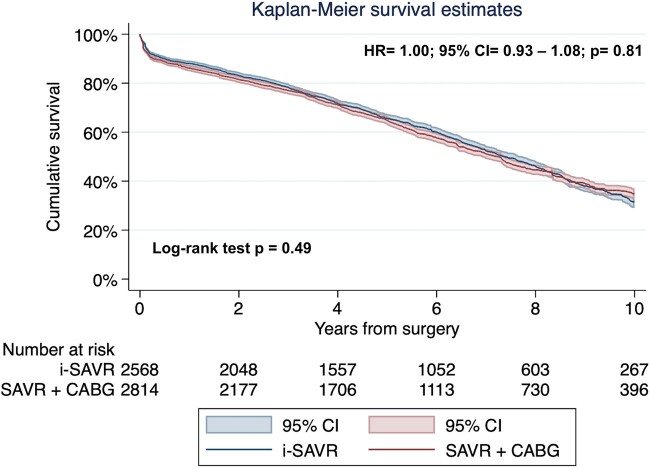
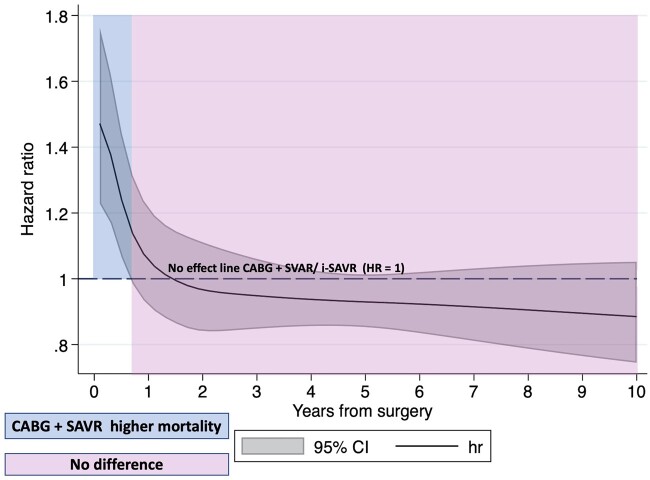
The long-term results in studies comparing octogenarian patients who received either isolated surgical aortic valve replacement (i-SAVR) or coronary artery bypass grafting (CABG) in addition to SAVR are still debated. We performed a reconstructed time-to-event data meta-analysis of studies comparing i-SAVR and CABG+SAVR to evaluate the impact of CABG and to analyse the time-varying effects on long-term outcome. We performed a systematic review of the literature from January 2000 through November 2021, including studies comparing i-SAVR and CABG+SAVR, which reported at least 3-year follow-up and that plotted Kaplan-Meier curves of overall survival. The primary endpoint was overall long-term survival; secondary endpoints were in-hospital/30-day mortality and postoperative outcomes. The pooled hazard ratio (HR) and odds ratio) with 95% confidence interval (CI) were calculated for primary and secondary endpoints, respectively. Random-effect model was used in all analyses. Sixteen retrospective studies were included (5382 patients, i-SAVR = 2568 and CABG+SAVR = 2814). I-SAVR showed a lower incidence of in-hospital mortality compared to CABG+SAVR (odds ratio = 0.73; 95% CI= 0.60-0.89; P = 0.002). Landmark analyses showed a significantly higher all-cause mortality within 1 year from surgery in CABG+SAVR (HR = 1.17; 95% CI = 1.01-1.36; P = 0.03); after 1 year, no significant difference was observed (HR = 0.95; 95% CI = 0.87-1.04; P = 0.35). Landmark analysis was confirmed by time-varying trend of HR. Late survival of octogenarians did not differ significantly between the 2 interventions. Interestingly, CABG added to SAVR was associated with both higher in-hospital and within 1-year mortality after surgery, whereas this difference was statistically non-significant at long-term follow-up.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


