Sarah Small, Rachael Coulson, Robert Spence, Ian McAllister
{"title":"Is qFIT a useful tool in prioritising symptomatic patients referred with suspect colorectal cancer in the COVID-19 era?","authors":"Sarah Small, Rachael Coulson, Robert Spence, Ian McAllister","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The COVID-19 pandemic is an evolving healthcare challenge causing secondary disruption of cancer services. Quantitative Faecal Immunochemical Testing (qFIT) has been established as a screening method in asymptomatic patients. We aim to assess its utility as a triage tool to prioritise investigations in symptomatic patients with suspected colorectal cancer.</p><p><strong>Methods: </strong>At the commencement of the COVID-19 pandemic a database was established to include patients awaiting red flag outpatient consultation or colonic investigations and new red flag referrals from March to June 2020. Patients were supplied with qFIT kits and returned results categorised into 3 priority groups according to the qFIT value. Group 1 >150µg Hb/g, Group 2 ≥10 to ≤150µg Hb/g and Group 3 <10µg Hb/g. Subsequent colonic evaluation was offered by colonoscopy or cross-sectional imaging with urgency determined by qFIT priority group. When identified colorectal cancer, inflammatory bowel disease or high-risk polyps were recorded as \"significant colorectal pathology.\"</p><p><strong>Findings: </strong>Three hundred and seventeen patients were identified with data analysed on 290 patients. Colorectal malignancy was identified in 17 patients; 94% of these patients were in Group 1. A qFIT result >150 µg Hb/g had a sensitivity and specificity for colorectal cancer of 94.12% (95% CI 71.31-99.85) and 91.21% (95% CI 87.20-94.29) respectively. No malignancy was detected in Priority Group 3; negative predictive value of 100% (95% CI 98.06-100).</p><p><strong>Conclusions: </strong>In symptomatic, suspect lower GI cancer patients qFIT is a useful adjunct for prioritising patients and can be used to determine the urgency of colorectal investigations.</p>","PeriodicalId":38815,"journal":{"name":"Ulster Medical Journal","volume":" ","pages":"79-84"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/27/e7/umj-91-02-79.PMC9200097.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulster Medical Journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The COVID-19 pandemic is an evolving healthcare challenge causing secondary disruption of cancer services. Quantitative Faecal Immunochemical Testing (qFIT) has been established as a screening method in asymptomatic patients. We aim to assess its utility as a triage tool to prioritise investigations in symptomatic patients with suspected colorectal cancer.
Methods: At the commencement of the COVID-19 pandemic a database was established to include patients awaiting red flag outpatient consultation or colonic investigations and new red flag referrals from March to June 2020. Patients were supplied with qFIT kits and returned results categorised into 3 priority groups according to the qFIT value. Group 1 >150µg Hb/g, Group 2 ≥10 to ≤150µg Hb/g and Group 3 <10µg Hb/g. Subsequent colonic evaluation was offered by colonoscopy or cross-sectional imaging with urgency determined by qFIT priority group. When identified colorectal cancer, inflammatory bowel disease or high-risk polyps were recorded as "significant colorectal pathology."
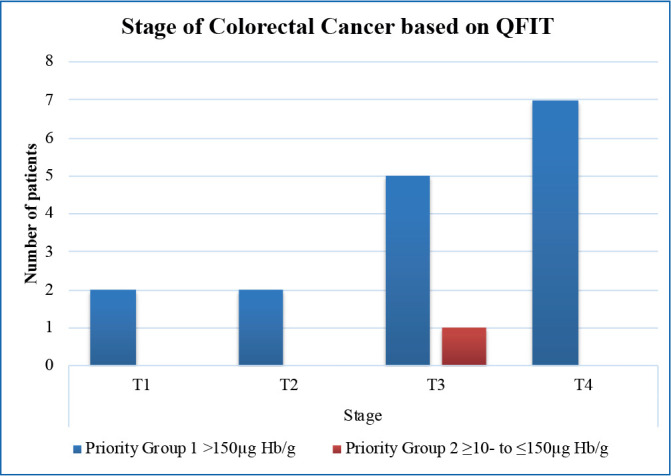
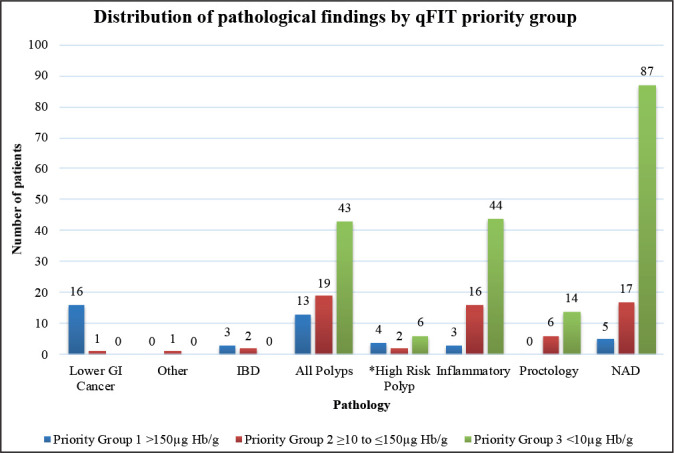
Findings: Three hundred and seventeen patients were identified with data analysed on 290 patients. Colorectal malignancy was identified in 17 patients; 94% of these patients were in Group 1. A qFIT result >150 µg Hb/g had a sensitivity and specificity for colorectal cancer of 94.12% (95% CI 71.31-99.85) and 91.21% (95% CI 87.20-94.29) respectively. No malignancy was detected in Priority Group 3; negative predictive value of 100% (95% CI 98.06-100).
Conclusions: In symptomatic, suspect lower GI cancer patients qFIT is a useful adjunct for prioritising patients and can be used to determine the urgency of colorectal investigations.
背景:COVID-19大流行是一项不断演变的卫生保健挑战,导致癌症服务的二次中断。定量粪便免疫化学试验(qFIT)已被确立为无症状患者的筛查方法。我们的目的是评估其作为一种分类工具的效用,优先调查有症状的疑似结直肠癌患者。方法:在COVID-19大流行开始时建立数据库,包括2020年3月至6月等待红旗门诊或结肠调查的患者和新的红旗转诊患者。为患者提供qFIT试剂盒,并根据qFIT值将返回的结果分为3个优先组。第1组>150µg Hb/g,第2组≥10至≤150µg Hb/g,第3组结果:共鉴定出317例患者,分析了290例患者的数据。结直肠恶性肿瘤17例;其中94%的患者为第一组。qFIT结果>150µg Hb/g对结直肠癌的敏感性和特异性分别为94.12% (95% CI 71.31-99.85)和91.21% (95% CI 87.20-94.29)。优先组3未见恶性肿瘤;阴性预测值为100% (95% CI 98.06-100)。结论:在有症状的可疑下消化道肿瘤患者中,qFIT是确定患者优先级的有用辅助手段,可用于确定结直肠检查的紧迫性。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


