{"title":"Quadriceps muscle volume has no effect on patellofemoral cartilage lesions in patients with end-stage knee osteoarthritis.","authors":"Jung-Ro Yoon, Hong Joon Joo, Seung Hoon Lee","doi":"10.1186/s43019-022-00134-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The quadriceps muscle has a positive effect on anterior knee pain. However, its effect on the patellofemoral (PF) cartilage in patients with end-stage knee osteoarthritis is unknown. The present study aimed to evaluate whether the quadriceps muscle area had a positive effect on the PF cartilage and whether this muscle had a positive effect on the clinical scores.</p><p><strong>Materials and methods: </strong>Patients with confirmed cartilage status and clinical scores who underwent total knee arthroplasty (TKA) were included. The PF cartilage status was evaluated during TKA. The thickness and the area of the quadriceps muscle were measured using a knee computed tomography scan obtained before the surgery. The Q-angle, hip-knee-ankle angle, alignment, and Insall-Salvati ratio were measured by radiography.</p><p><strong>Results: </strong>Altogether, 204 patients were included in the study. Logistic regression was performed including factors associated with PF cartilage lesions. The regression model was found to be statistically significant (Hosmer-Lemeshow test, χ<sup>2</sup> = 0.493). A smaller hip-knee-ankle (HKA) angle was associated with a higher incidence of PF cartilage lesions (p = 0.033) and only the alignment had an effect on the PF cartilage lesions. PF cartilage lesions did not correlate with the clinical scores. A thicker medial portion of the quadriceps muscle was associated with a significantly higher Knee Society Knee Score (KSKS) (p = 0.028).</p><p><strong>Conclusions: </strong>Quadriceps muscle thickness and area, Q-angle, and patellar height were not associated with PF cartilage lesions, while a smaller HKA angle was associated with PF cartilage lesions. The presence of PF cartilage lesions did not affect the clinical symptoms. However, a thicker medial portion of the quadriceps muscle was associated with a higher KSKS.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":" ","pages":"6"},"PeriodicalIF":4.4000,"publicationDate":"2022-02-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8858450/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-022-00134-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 3
Abstract
Purpose: The quadriceps muscle has a positive effect on anterior knee pain. However, its effect on the patellofemoral (PF) cartilage in patients with end-stage knee osteoarthritis is unknown. The present study aimed to evaluate whether the quadriceps muscle area had a positive effect on the PF cartilage and whether this muscle had a positive effect on the clinical scores.
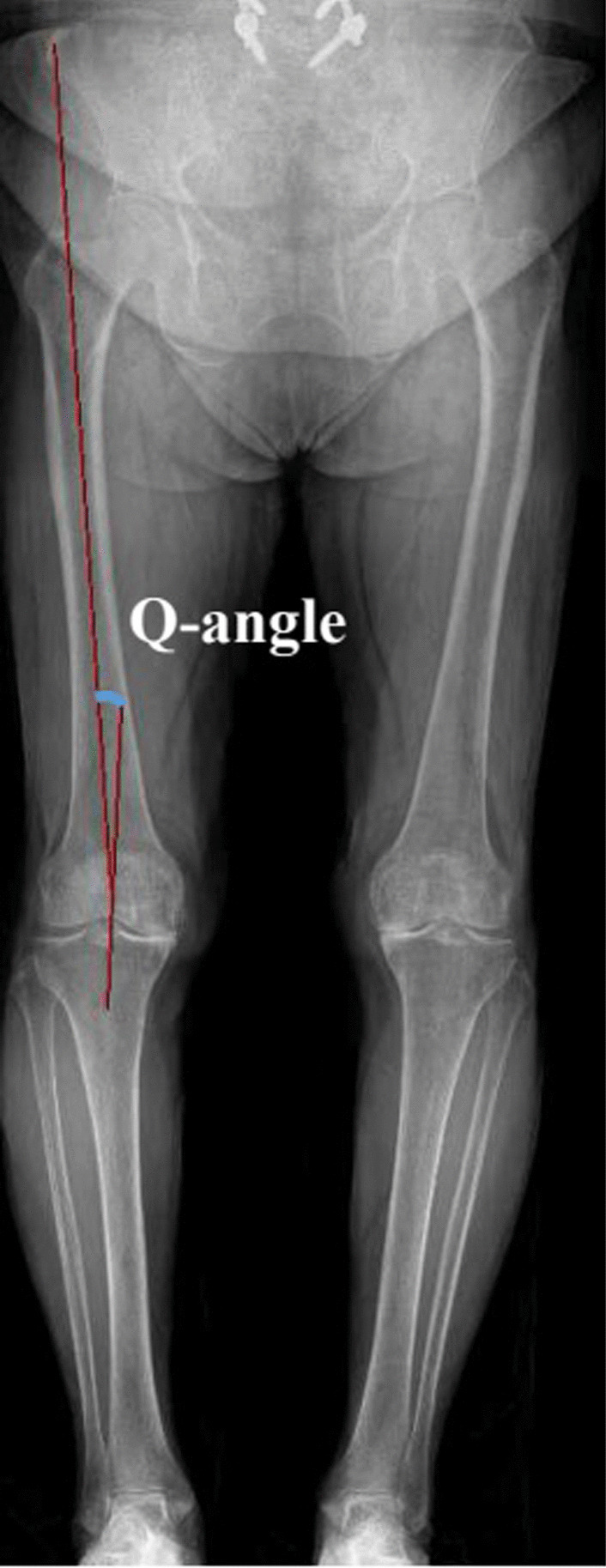
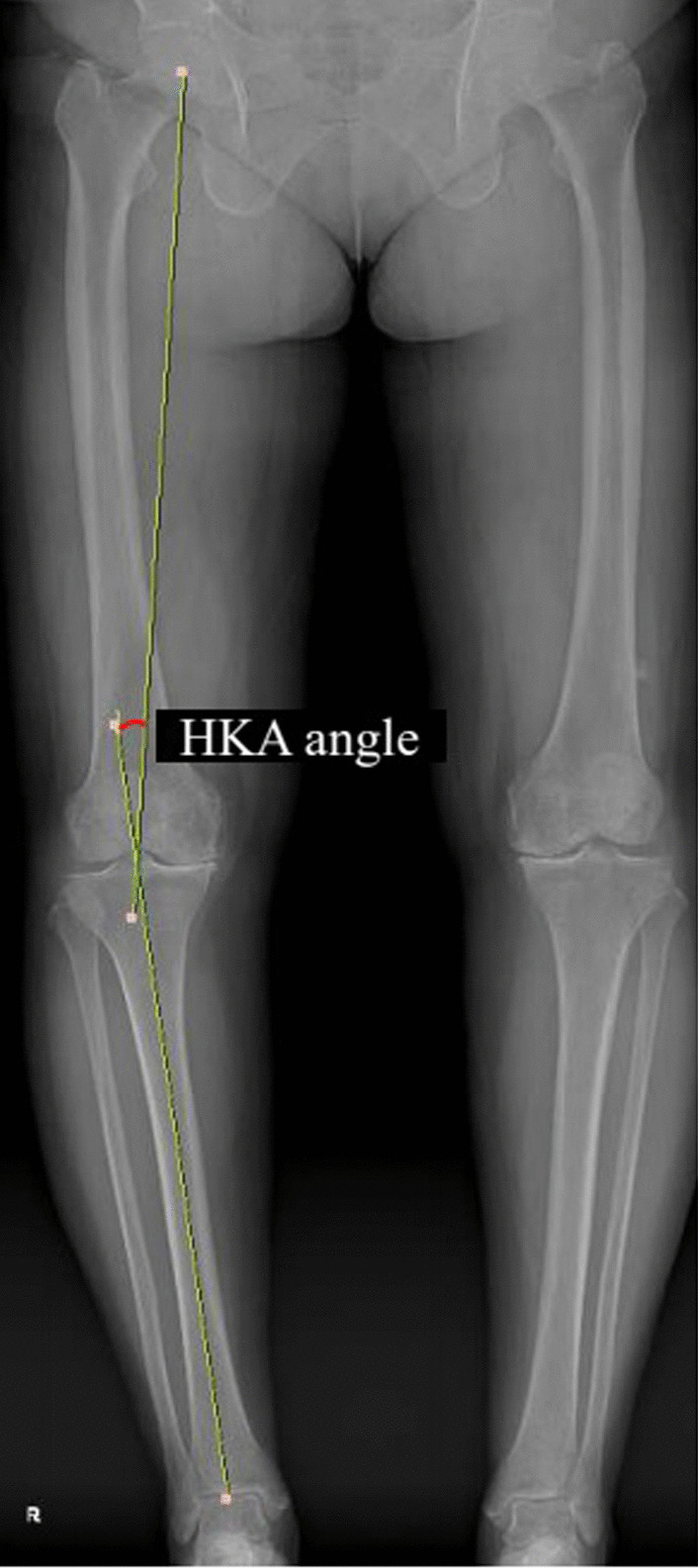
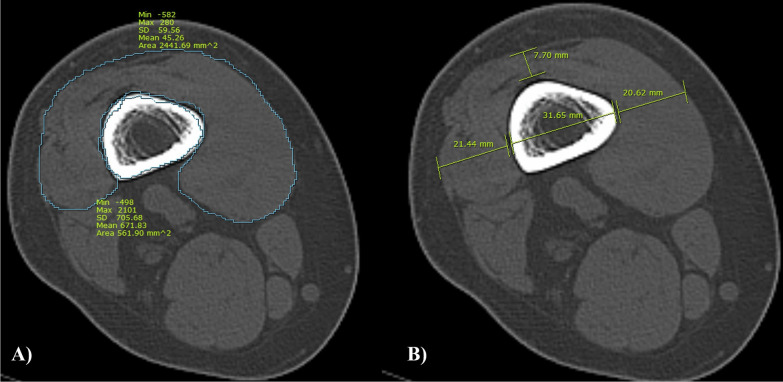
Materials and methods: Patients with confirmed cartilage status and clinical scores who underwent total knee arthroplasty (TKA) were included. The PF cartilage status was evaluated during TKA. The thickness and the area of the quadriceps muscle were measured using a knee computed tomography scan obtained before the surgery. The Q-angle, hip-knee-ankle angle, alignment, and Insall-Salvati ratio were measured by radiography.
Results: Altogether, 204 patients were included in the study. Logistic regression was performed including factors associated with PF cartilage lesions. The regression model was found to be statistically significant (Hosmer-Lemeshow test, χ2 = 0.493). A smaller hip-knee-ankle (HKA) angle was associated with a higher incidence of PF cartilage lesions (p = 0.033) and only the alignment had an effect on the PF cartilage lesions. PF cartilage lesions did not correlate with the clinical scores. A thicker medial portion of the quadriceps muscle was associated with a significantly higher Knee Society Knee Score (KSKS) (p = 0.028).
Conclusions: Quadriceps muscle thickness and area, Q-angle, and patellar height were not associated with PF cartilage lesions, while a smaller HKA angle was associated with PF cartilage lesions. The presence of PF cartilage lesions did not affect the clinical symptoms. However, a thicker medial portion of the quadriceps muscle was associated with a higher KSKS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


