Jae-Myung Kim, Kyung Wook Kang, Hyong-Ho Cho, Man-Seok Park, Seung-Han Lee
{"title":"Ramsay Hunt Syndrome Presenting as Acute Unilateral Combined Peripheral and Central Vestibulopathies.","authors":"Jae-Myung Kim, Kyung Wook Kang, Hyong-Ho Cho, Man-Seok Park, Seung-Han Lee","doi":"10.3988/jcn.2022.18.1.108","DOIUrl":null,"url":null,"abstract":"Dear Editor, A previously healthy 68-year-old female presented with spontaneous spinning vertigo with a 10-day history. She had been treated with intravenous acyclovir for 10 days before the onset of vertigo under a diagnosis of Ramsay Hunt syndrome (RHS). She denied otologic symptoms including hearing loss. The initial neurologic examinations revealed right-sided peripheral facial paralysis and spontaneous left-beating nystagmus (Fig. 1A). However, the direction of nystagmus shifted to the right side while looking toward the right, which suggested gazeevoked nystagmus (GEN) (Fig. 1A). Skew deviation was absent, but prominent right-sided veering tendency without limb ataxia was noted. Bedside head impulse tests (HITs) revealed abnormal catch-up saccades (CS) in the right. Bithermal caloric testing demonstrated right-canal paresis. However, video HITs showed decreases in the vestibulo-ocular reflex (VOR) gains in all six semicircular canals, with rightsided predominance (Fig. 1B and C). Cervical and ocular vestibular-evoked myogenic potentials were not observed when stimulating the right ear. Pure-tone audiometry was normal. GEN, bilateral abnormalities in video HITs, and severe prolonged vertigo with prominent imbalance were suggestive of a central vestibulopathy. Gadolinium-enhanced brain magnetic resonance imaging (MRI) revealed enhanced lesions in the brainstem (Fig. 1D-G). Therefore, a presumptive diagnosis of RHS with brainstem involvement was made based on the clinical and neuroradiologic findings. The addition of intravenous administration of dexamethasone and acyclovir for 7 days improved all of the symptoms except the facial paralysis. Patients with RHS often suffer from severe vertigo and/or otologic symptoms since the vestibulocochlear nerve is the most frequently involved cranial nerve.1,2 Accordingly, patients with RHS and vertigo typically present with acute peripheral vestibulopathy. However, RHS can be complicated by rare but serious central vestibular disorders involving the brainstem and/or cerebellum.3,4 Identifying central signs was essential for the correct diagnosis in our patient because she required additional treatment after discerning the central lesion.1 Our patient demonstrated clinical and laboratory features of combined peripheral and central vestibulopathies. A previous study of the etiologies and diagnoses of 55 patients with combined peripheral and central vestibulopathies identified only 1 case of RHS.4 That patient exhibited GEN as a central sign and other presentations consistent with unilateral peripheral vestibulopathy, but brain MRI was normal, in contrast to our case. There have been few studies of the neuro-otologic and vestibular evaluations in RHS with brainstem involvement.1 Dissociation in the VOR between different stimulation frequencies could be a significant feature of combined vestibulopathy.4 Our patient showed ipsilesional (unilateral) canal paresis in the caloric test (low-frequency VOR), but bilaterally decreased VOR gains with abnormal CS in the video HITs (high-frequency VOR). In cases involving central vestibular structures including the vestibular nucleus, nucleus prepositus hypoglossi (NPH), or flocculus, a disruption in neural interconnection between the structures may result in a reduction in VOR gains Jae-Myung Kim Kyung Wook Kang Hyong-Ho Cho Man-Seok Park Seung-Han Lee","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"108-110"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e4/0b/jcn-18-108.PMC8762492.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.1.108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
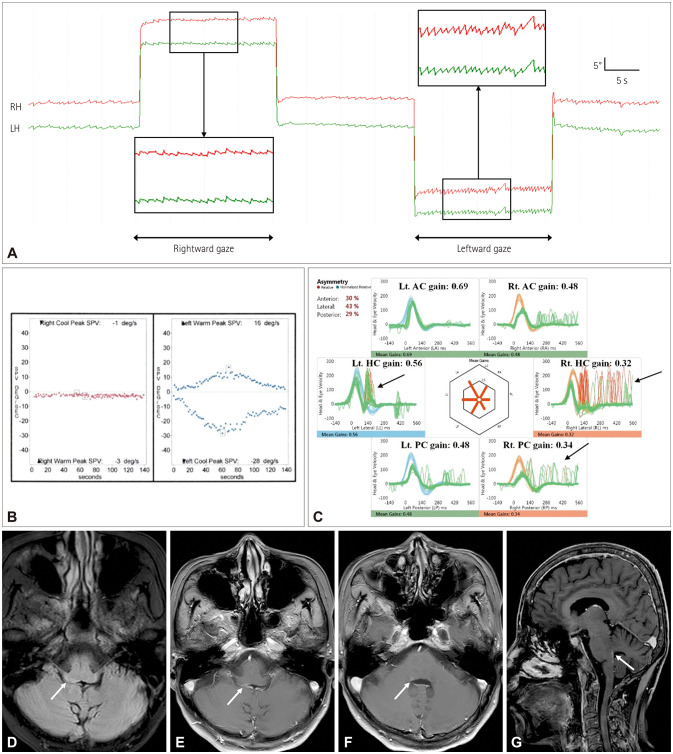
Dear Editor, A previously healthy 68-year-old female presented with spontaneous spinning vertigo with a 10-day history. She had been treated with intravenous acyclovir for 10 days before the onset of vertigo under a diagnosis of Ramsay Hunt syndrome (RHS). She denied otologic symptoms including hearing loss. The initial neurologic examinations revealed right-sided peripheral facial paralysis and spontaneous left-beating nystagmus (Fig. 1A). However, the direction of nystagmus shifted to the right side while looking toward the right, which suggested gazeevoked nystagmus (GEN) (Fig. 1A). Skew deviation was absent, but prominent right-sided veering tendency without limb ataxia was noted. Bedside head impulse tests (HITs) revealed abnormal catch-up saccades (CS) in the right. Bithermal caloric testing demonstrated right-canal paresis. However, video HITs showed decreases in the vestibulo-ocular reflex (VOR) gains in all six semicircular canals, with rightsided predominance (Fig. 1B and C). Cervical and ocular vestibular-evoked myogenic potentials were not observed when stimulating the right ear. Pure-tone audiometry was normal. GEN, bilateral abnormalities in video HITs, and severe prolonged vertigo with prominent imbalance were suggestive of a central vestibulopathy. Gadolinium-enhanced brain magnetic resonance imaging (MRI) revealed enhanced lesions in the brainstem (Fig. 1D-G). Therefore, a presumptive diagnosis of RHS with brainstem involvement was made based on the clinical and neuroradiologic findings. The addition of intravenous administration of dexamethasone and acyclovir for 7 days improved all of the symptoms except the facial paralysis. Patients with RHS often suffer from severe vertigo and/or otologic symptoms since the vestibulocochlear nerve is the most frequently involved cranial nerve.1,2 Accordingly, patients with RHS and vertigo typically present with acute peripheral vestibulopathy. However, RHS can be complicated by rare but serious central vestibular disorders involving the brainstem and/or cerebellum.3,4 Identifying central signs was essential for the correct diagnosis in our patient because she required additional treatment after discerning the central lesion.1 Our patient demonstrated clinical and laboratory features of combined peripheral and central vestibulopathies. A previous study of the etiologies and diagnoses of 55 patients with combined peripheral and central vestibulopathies identified only 1 case of RHS.4 That patient exhibited GEN as a central sign and other presentations consistent with unilateral peripheral vestibulopathy, but brain MRI was normal, in contrast to our case. There have been few studies of the neuro-otologic and vestibular evaluations in RHS with brainstem involvement.1 Dissociation in the VOR between different stimulation frequencies could be a significant feature of combined vestibulopathy.4 Our patient showed ipsilesional (unilateral) canal paresis in the caloric test (low-frequency VOR), but bilaterally decreased VOR gains with abnormal CS in the video HITs (high-frequency VOR). In cases involving central vestibular structures including the vestibular nucleus, nucleus prepositus hypoglossi (NPH), or flocculus, a disruption in neural interconnection between the structures may result in a reduction in VOR gains Jae-Myung Kim Kyung Wook Kang Hyong-Ho Cho Man-Seok Park Seung-Han Lee

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


