Markus Gschwind, Barbora Zima, Krassen Nedeltchev, Pieter van Mierlo, Stephan Rüegg
{"title":"Tracking Multifocal Epilepsy With Automated Electric Source Imaging in a Patient With Triple-X Syndrome.","authors":"Markus Gschwind, Barbora Zima, Krassen Nedeltchev, Pieter van Mierlo, Stephan Rüegg","doi":"10.3988/jcn.2022.18.1.96","DOIUrl":null,"url":null,"abstract":"Dear Editor, Pharmacoresistant epilepsy with polymorphic behavior remains a great challenge in clinical epileptology. Here we present a 20-year-old female with triple-X syndrome who was admitted because of variable seizures and the suspicion of nonepileptic events. Absences with deep breathing, wagging of the left arm, yawning, nausea, aggressiveness, and amnesia were replaced by turning the head to the left, stretching the left arm, and bending the right arm (“figure-of-4 sign”), followed by confusion. Similar seizures occurred up to seven times per day on up to 20 days per month, resulting in numerous consultations at the emergency department. Tonic-clonic seizures had occurred during her 3rd year of life, and at 8 years old she started to also show focal nonaware cognitive seizures, sometimes with bilateral spread. At that time, several routine electroencephalography (EEG) recordings revealed a right, paracentral epileptic focus. Valproic acid (1,500 mg daily) resulted in a seizure-free period of 6 years, but this had to be discontinued due to weight gain and hirsutism, and was subsequently changed to levetiracetam (2,000 mg daily), lamotrigine (100 mg daily), and lacosamide (200 mg daily), which failed to control the seizures and increased behavioral problems. Brain magnetic resonance imaging (MRI) findings were normal. The patient underwent long-term overnight video-EEG with a 25-channel montage (2017 IFCN guidelines), which revealed several epileptogenic foci with sharp waves in the right inferotemporal (T10–F10) region, in the right central region at C4–P4, and in the left central region (C3–P3) (Fig. 1A-C). We then ran the fully automatic EPILOG PreOp algorithm (Epilog NV, Ghent, Belgium) in order to quantify the interictal epileptic discharges and localize their electric source according to the patient’s own brain anatomy (Fig. 1D-F). To this end, we used the full 88-hour-long low-density EEG track together with the patient’s own 3-T magnetization prepared rapid gradient echo MRI scan, allowing for an anatomical head model with six tissue compartments (gray matter, white matter, CSF, skull, air cavities, and scalp). The electrode positions were estimated by calculating distances over the head after marking specific landmarks such as the inion, nasion, and auricular points.1,2 EEG source analysis was done using sLORETA as the inverse technique to localize each spike according to its onset, half height, and peak. A patient-specific head model was constructed from the MRI data, and the finite-difference method was used to calculate the lead fields that linked neuronal currents in the brain to the measured scalp potentials.1,2 After demonstrating the presence of multifocal epilepsy in our patient, we changed the pharmacologic treatment to brivaracetam (100 mg daily), higher-dose lamotrigine (500 mg daily, serum level of 8.7 mg/L; ref. 3–14 mg/L), and low-dose valproic acid (300 mg daily), which subsequently resulted in a remarkable improvement of seizure control. Overnight video-EEG combined with fully automated electric source imaging was successful in confirming the hypothesis of different epileptic foci causing the changing seizure semiologies in our patient. The previously reported triple-X aberration additionally orientMarkus Gschwind Barbora Zima Krassen Nedeltchev Pieter van Mierlo Stephan Rüegg","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"96-98"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d7/67/jcn-18-96.PMC8762506.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.1.96","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
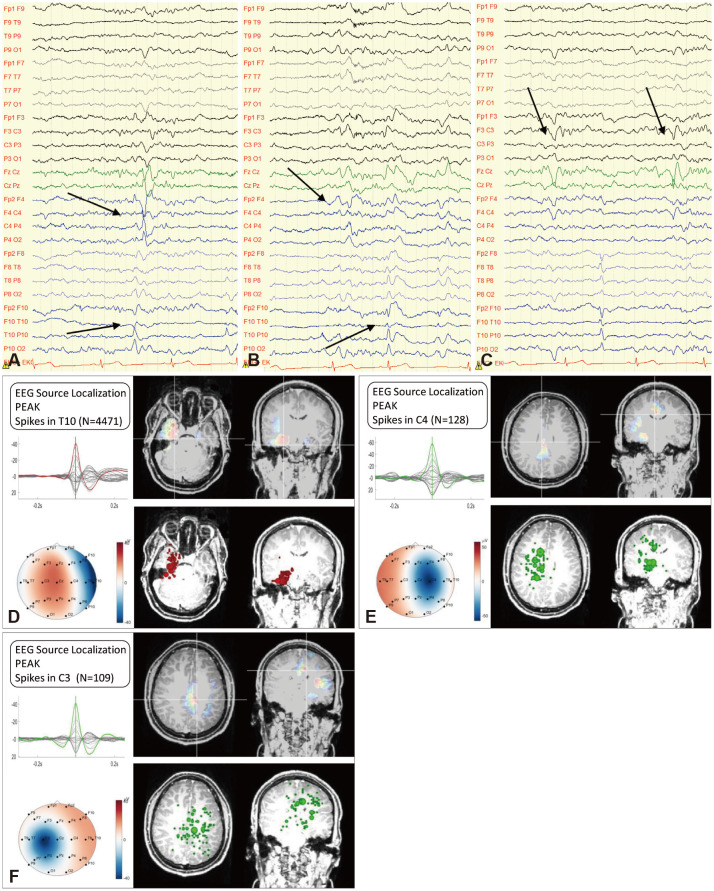
Dear Editor, Pharmacoresistant epilepsy with polymorphic behavior remains a great challenge in clinical epileptology. Here we present a 20-year-old female with triple-X syndrome who was admitted because of variable seizures and the suspicion of nonepileptic events. Absences with deep breathing, wagging of the left arm, yawning, nausea, aggressiveness, and amnesia were replaced by turning the head to the left, stretching the left arm, and bending the right arm (“figure-of-4 sign”), followed by confusion. Similar seizures occurred up to seven times per day on up to 20 days per month, resulting in numerous consultations at the emergency department. Tonic-clonic seizures had occurred during her 3rd year of life, and at 8 years old she started to also show focal nonaware cognitive seizures, sometimes with bilateral spread. At that time, several routine electroencephalography (EEG) recordings revealed a right, paracentral epileptic focus. Valproic acid (1,500 mg daily) resulted in a seizure-free period of 6 years, but this had to be discontinued due to weight gain and hirsutism, and was subsequently changed to levetiracetam (2,000 mg daily), lamotrigine (100 mg daily), and lacosamide (200 mg daily), which failed to control the seizures and increased behavioral problems. Brain magnetic resonance imaging (MRI) findings were normal. The patient underwent long-term overnight video-EEG with a 25-channel montage (2017 IFCN guidelines), which revealed several epileptogenic foci with sharp waves in the right inferotemporal (T10–F10) region, in the right central region at C4–P4, and in the left central region (C3–P3) (Fig. 1A-C). We then ran the fully automatic EPILOG PreOp algorithm (Epilog NV, Ghent, Belgium) in order to quantify the interictal epileptic discharges and localize their electric source according to the patient’s own brain anatomy (Fig. 1D-F). To this end, we used the full 88-hour-long low-density EEG track together with the patient’s own 3-T magnetization prepared rapid gradient echo MRI scan, allowing for an anatomical head model with six tissue compartments (gray matter, white matter, CSF, skull, air cavities, and scalp). The electrode positions were estimated by calculating distances over the head after marking specific landmarks such as the inion, nasion, and auricular points.1,2 EEG source analysis was done using sLORETA as the inverse technique to localize each spike according to its onset, half height, and peak. A patient-specific head model was constructed from the MRI data, and the finite-difference method was used to calculate the lead fields that linked neuronal currents in the brain to the measured scalp potentials.1,2 After demonstrating the presence of multifocal epilepsy in our patient, we changed the pharmacologic treatment to brivaracetam (100 mg daily), higher-dose lamotrigine (500 mg daily, serum level of 8.7 mg/L; ref. 3–14 mg/L), and low-dose valproic acid (300 mg daily), which subsequently resulted in a remarkable improvement of seizure control. Overnight video-EEG combined with fully automated electric source imaging was successful in confirming the hypothesis of different epileptic foci causing the changing seizure semiologies in our patient. The previously reported triple-X aberration additionally orientMarkus Gschwind Barbora Zima Krassen Nedeltchev Pieter van Mierlo Stephan Rüegg

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


